New Oral Anticoagulant Therapy Versus Warfarin In Patients With Atrial Fibrillation And Previous Stroke or Transient Ischemic Attack. An Updated Meta-analysis.
Abstract Body: Background: Patients with atrial fibrillation (AF) and previous stroke or transient ischemic attack (TIA) are at high risk of recurrent stroke. Data regarding the efficacy and safety of new oral anticoagulant therapy (NOAC) compared to warfarin in patients with previous strokes are lacking.
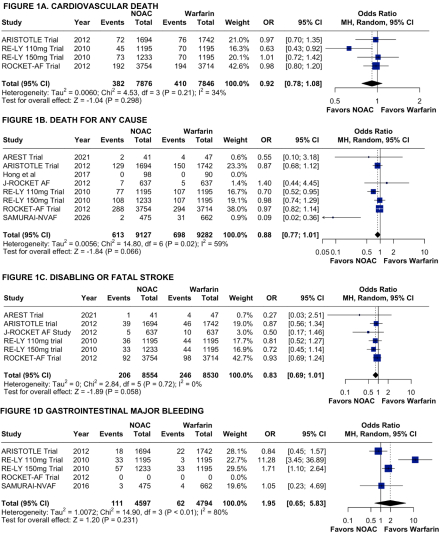
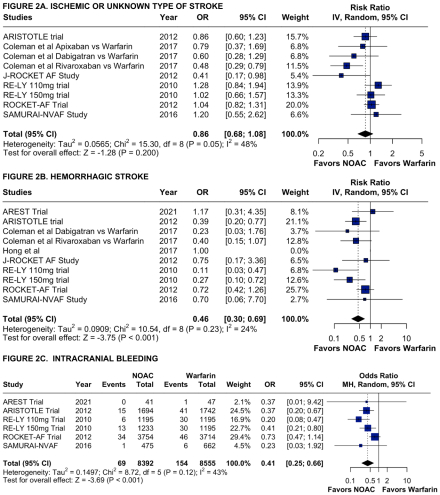
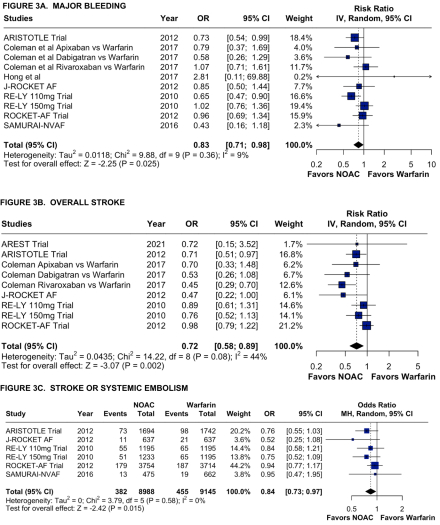
Method: PubMed, Scopus and Cochrane databases were searched for both randomized controlled trials (RCTs) and non-randomized controlled trials (non-RCTs) that compared NOAC to warfarin in patients with AF and previous stroke or TIA and that reported the outcomes of cardiovascular death, death from any cause, disabling or fatal stroke, gastrointestinal major bleeding, hemorrhagic stroke, intracranial bleeding, major bleeding, overall stroke etc. Heterogeneity was examined using I2 statistics.
Results: We included 7 RCTs and 2 non-RCTs comparing NOAC to warfarin in patients with atrial fibrillation and previous stroke or TIA. The pooled results showed that cardiovascular death (4.9% vs 5.2% respectively; OR = 0.92; 95% CI [0.78, 1.08]; I2 = 34%; p = 0.298), death from any cause (6.7% vs 7.5% respectively; OR = 0.88; 95% CI [0.77, 1.01]; I2 = 59%; p = 0.066), disabling or fatal stroke (2.4% vs 2.9% respectively; OR = 0.83; 95% CI [0.69, 1.01]; I2 = 0%; p = 0.058), gastrointestinal major bleeding (2.4% vs 1.3% respectively; OR = 1.95; 95% CI [0.65, 5.83]; I2 = 80%; p = 0.231), and ischemic or unknown type of stroke (RR = 0.86; 95% CI [0.69, 1.08]; I2 = 48%; p = 0.200) are not statistically different between the NAOC group and warfarin group. However, hemorrhagic stroke (RR = 0.46; 95% CI [0.30, 0.69]; I2 = 24%; p < 0.001), intracranial bleeding (0.82% vs 1.8% respectively; OR = 0.41; 95% CI [0.25, 0.66]; I2 = 43%; p < 0.001), major bleeding (RR = 0.83; 95% CI [0.71, 0.98]; I2 = 9%; p = 0.025), overall stroke (RR = 0.72; 95% CI [0.58, 0.89]; I2 = 44%; p = 0.002) and stroke or systemic embolism (4.3% vs 5.0% respectively; OR = 0.84; 95% CI [0.73, 0.97]; I2 = 0%; p = 0.015) are significantly reduced in the NAOC group compared to the warfarin group.
Conclusion: In patients with atrial fibrillation and previous stroke or transient ischemic attack, treatment with NOAC did not show any significant difference compared with warfarin for outcomes of death from any cause, cardiovascular death, disabling or fatal stroke, and gastrointestinal major bleeding. NOAC reduces the risk of hemorrhagic stroke, intracranial bleeding, major bleeding, and overall stroke compared to warfarin.
Obi, Ogechukwu
(
New York Institute of Technology College of Osteopathic Medicine
, Glen Head , New York , United States )
Cavalcante, Deivyd
(
Federal University of Maranhao
, Sao Luis , Brazil )
Nweze, Uchenna
(
University of Massachusetts Global
, Aliso Viejo , California , United States )
Asonye, Patricia
(
UIC College of Pharmacy
, Chicago , Illinois , United States )
Lee, Timothy
(
Optum
, Roslyn Heights , New York , United States )
Author Disclosures:
OGECHUKWU OBI:DO NOT have relevant financial relationships
| Deivyd Cavalcante:DO NOT have relevant financial relationships
| Uchenna Nweze:DO NOT have relevant financial relationships
| Patricia Asonye:DO NOT have relevant financial relationships
| Timothy Lee:No Answer