Digital Access and Cardiovascular Health: Evidence from the Roots of Wellness Trial Baseline Data
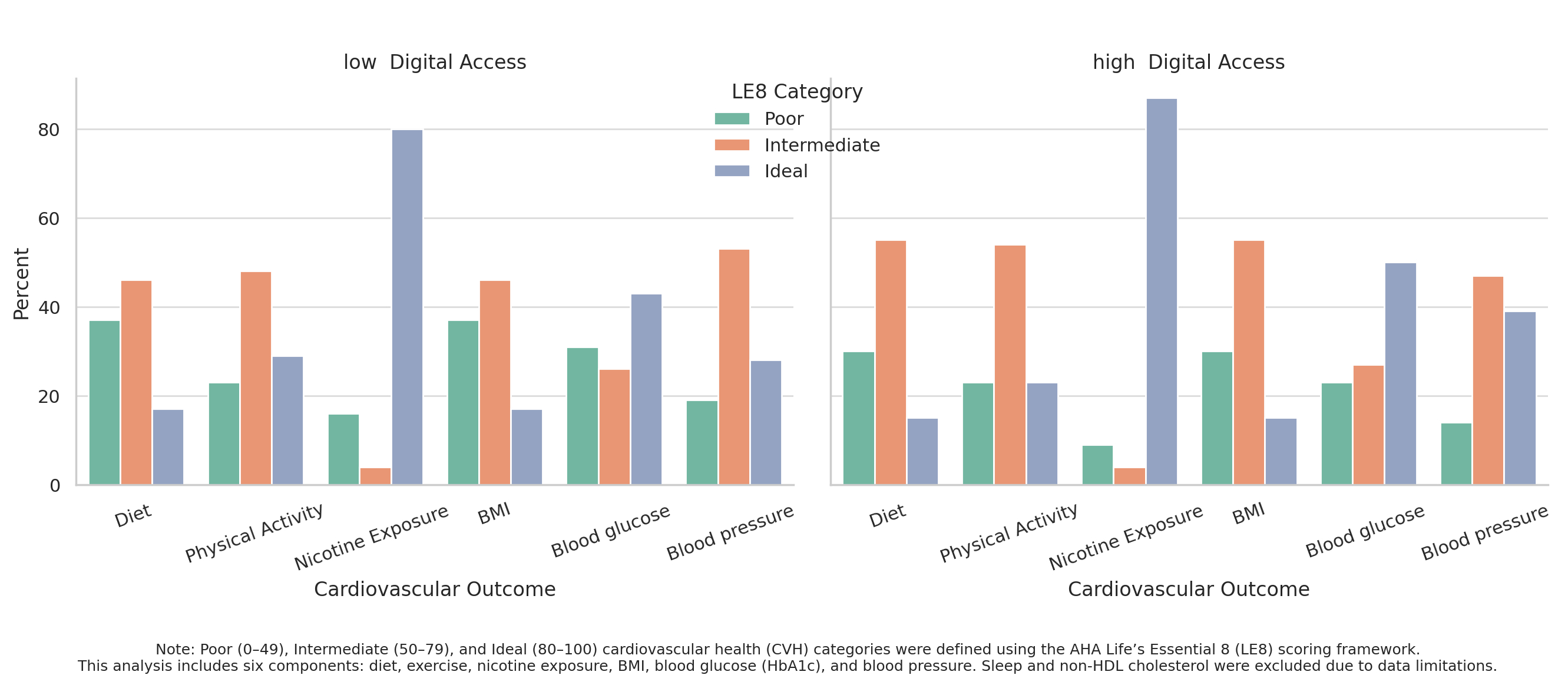
Abstract Body: Background: Black and Latino adults experience a greater burden of cardiovascular disease than other U.S. populations. Digital access and digital health literacy may help improve cardiovascular outcomes in these populations. Objective: To examine associations between digital access, digital health literacy, and composite cardiovascular health (CVH) scores. A secondary objective was to assess whether access to care and social services moderated these associations. Methods: We conducted a cross-sectional analysis using baseline data from the Roots of Wellness randomized controlled trial (N=339) in Maryland and Washington, D.C. Digital health literacy was measured using 10 items from the Digital Health Literacy Inventory (range: 10–40). Digital access was assessed using an 11-point composite score capturing device ownership, internet use, and digital skills. Covariates included age, education, and income. Moderators included social-emotional support, delayed care due to cost, and insurance. Multivariable linear regression models examined associations between digital health literacy, digital access, and CVH, with interaction terms included. A modified CVH score was computed using six of the Life’s Essential 8 components: diet, smoking, physical activity, BMI, hemoglobin A1c, and blood pressure. Each was scored from 0 to 100 and averaged to create a composite score (range: 0–100). Results: Participants had a mean age of 53 years; 48% identified as Black and 52% as Latino. Most had a high school education or less (62%) and income under $35,000 (76%). Intermediate CVH scores (50–79) were observed in 64%. Half scored above the mean for digital health literacy and had digital access scores ≥8. A higher proportion of those with high digital access achieved ideal scores in nicotine exposure (87% vs. 80%), blood glucose (50% vs. 43%), and blood pressure (39% vs. 28%), though differences were not statistically significant. Digital access was significantly associated with increased CVH scores (β = 1.07, 95% CI: 0.66–1.49), though this was attenuated after adjusting for education. Digital health literacy was not associated with CVH scores. Social support, insurance, and delayed care did not moderate the digital access–CVH relationship. Conclusions: Digital access is associated with better CVH. Addressing disparities in digital access may help advance CVH equity in populations with a greater cardiovascular disease burden.
Chepkorir, Joyline
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Ogungbe, Bunmi
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Milller, Hailey
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Adomako, Nana
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Dennison Himmelfarb, Cheryl
(
JOHNS HOPKINS UNIV
, Baltimore , Maryland , United States )
Author Disclosures:
Joyline Chepkorir:DO NOT have relevant financial relationships
| Bunmi Ogungbe:DO NOT have relevant financial relationships
| HAILEY MILLLER:No Answer
| Nana Adomako:No Answer
| Cheryl Dennison Himmelfarb:DO NOT have relevant financial relationships
Jiang Chao, Dong Jianzeng, Cai Jun, Anderson Craig, Du Xin, Tang Yangyang, Han Rong, Song Yanna, Wang Chi, Lin Xiaolei, Yi Yang, Rodgers Anthony, Ma Changsheng