Timing of Antihypertensive Medications and Cardiovascular Outcomes: An Updated Meta-Analysis of Randomized Controlled Trials
Abstract Body: Introduction: Antihypertensive medications play a key role in improving cardiovascular (CV) outcomes, but the optimal time of day to administer these medications remains unclear. While two studies by Hermida et al. (2010, 2020) reported CV benefits with evening dosing, other trials have reported neutral results. This meta-analysis, which includes the most recent trial published by Garrison et al. (2025), reassesses the effect of antihypertensive dosing time on clinical CV outcomes.
Hypothesis: It was hypothesized that there would be no significant difference in all-cause mortality or major CV outcomes—myocardial infarction (MI), stroke, or heart failure—between morning and evening dosing of antihypertensive medications.
Methods: PubMed, Embase, and Cochrane CENTRAL were systematically searched from inception through May 2025 to identify randomized controlled trials (RCTs) comparing morning versus evening dosing of antihypertensive medications. Eligible studies included adult patients with hypertension and reported the following clinical outcomes: all-cause mortality, MI, stroke, or heart failure. Data was pooled using Review Manager (RevMan) version 5.4, and the Mantel-Haenszel odds ratio (OR) and 95% confidence interval (CI) were calculated using a random-effects model.
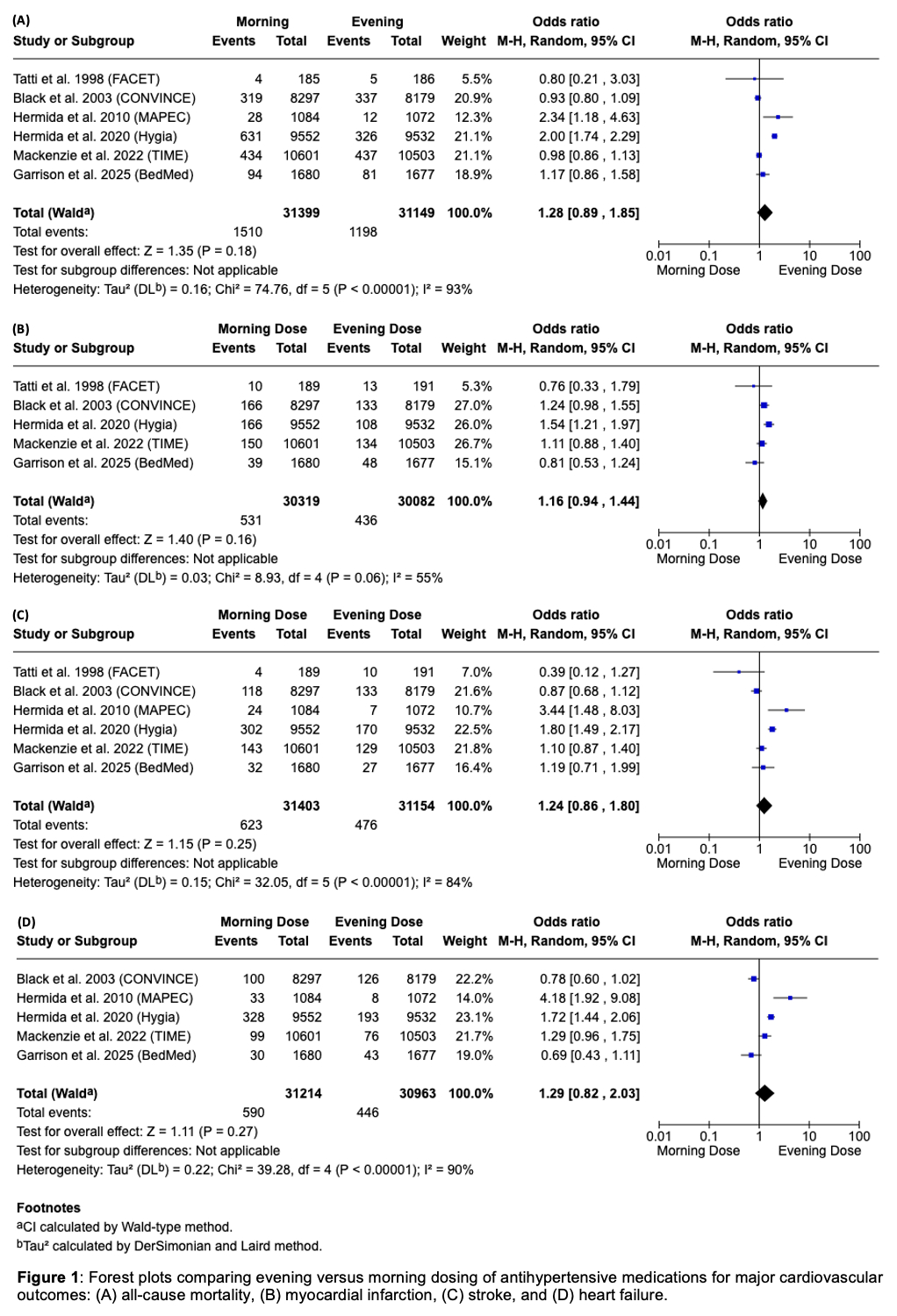
Results: Six RCTs comprising of 62,548 participants were included. Evening administration was not associated with a statistically significant reduction in all-cause mortality (OR = 1.28, CI 0.89–1.85, p = 0.18), MI (OR = 1.16, CI 0.94–1.44, p = 0.16), stroke (OR = 1.24, CI 0.86–1.80, p = 0.25), or heart failure (OR = 1.29, CI 0.82–2.03, p = 0.27) compared with morning dosing.
Conclusion: This meta-analysis found no significant difference between evening and morning dosing of antihypertensive medications in reducing all-cause mortality, MI, stroke, or heart failure. These results suggest that antihypertensive dosing time does not affect CV outcomes and can be individualized based on patient preference to optimize medication adherence. Future studies should explore specific patient subgroups and antihypertensive classes to identify any populations that may benefit from time-specific dosing.
Paul, Trishita
(
Tulane University
, New Orleans , Louisiana , United States )
Paul, Teebro
(
University of South Carolina
, Columbia , South Carolina , United States )
Bista, Roshan
(
Ascension Saint Thomas Heart
, Nashville , Tennessee , United States )
Mamudu, Hadii
(
East Tennessee State University
, Johnson City , Tennessee , United States )
Baljepally, Raj
(
University of Tennessee Medical Center
, Knoxville , Tennessee , United States )
Kerrigan, Jimmy
(
Ascension Saint Thomas Heart
, Nashville , Tennessee , United States )