Hypertensive Renal Disease Mortality in the United States (1999–2023): A 25-Year Analysis of Trends and Sociodemographic Disparities
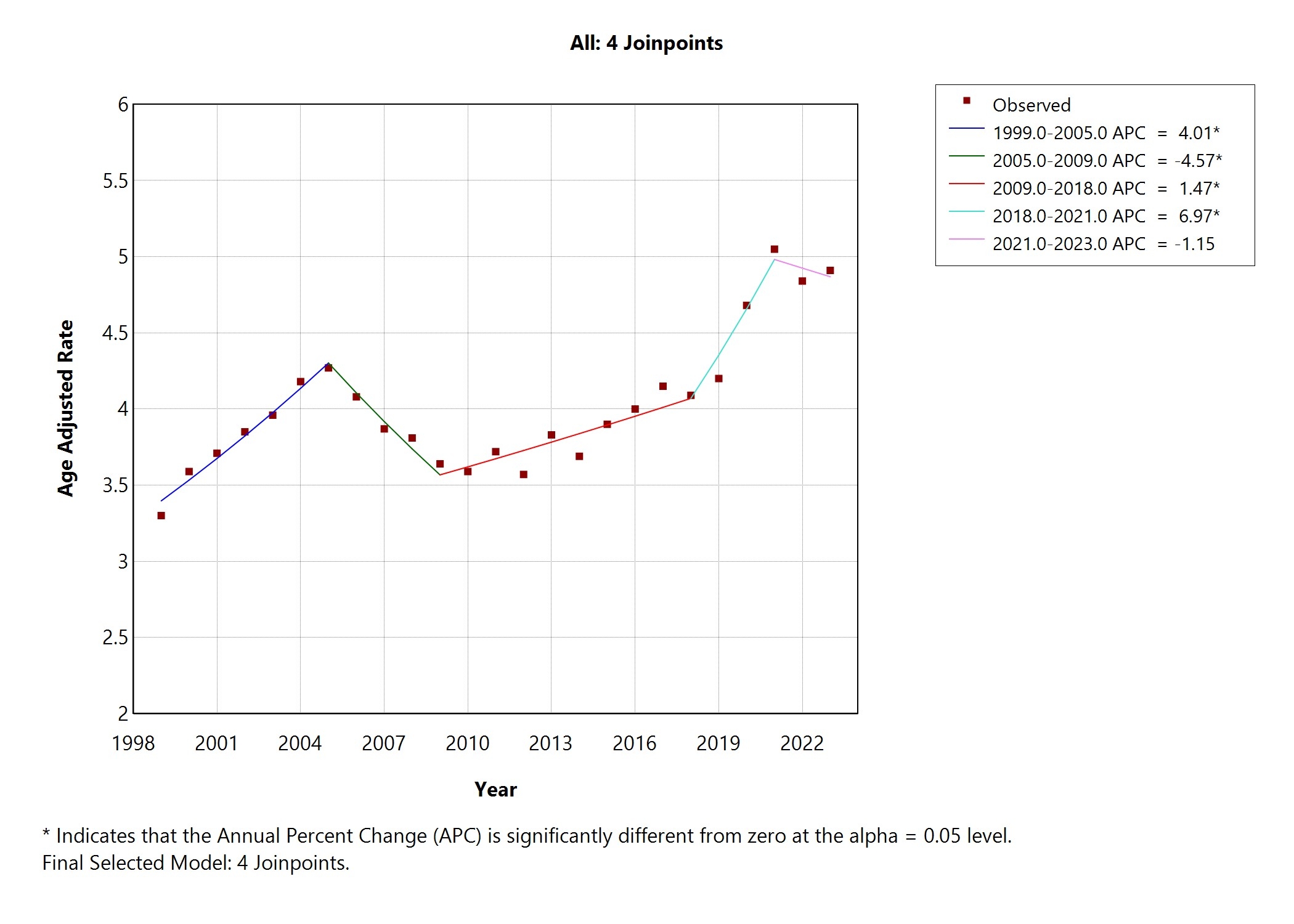
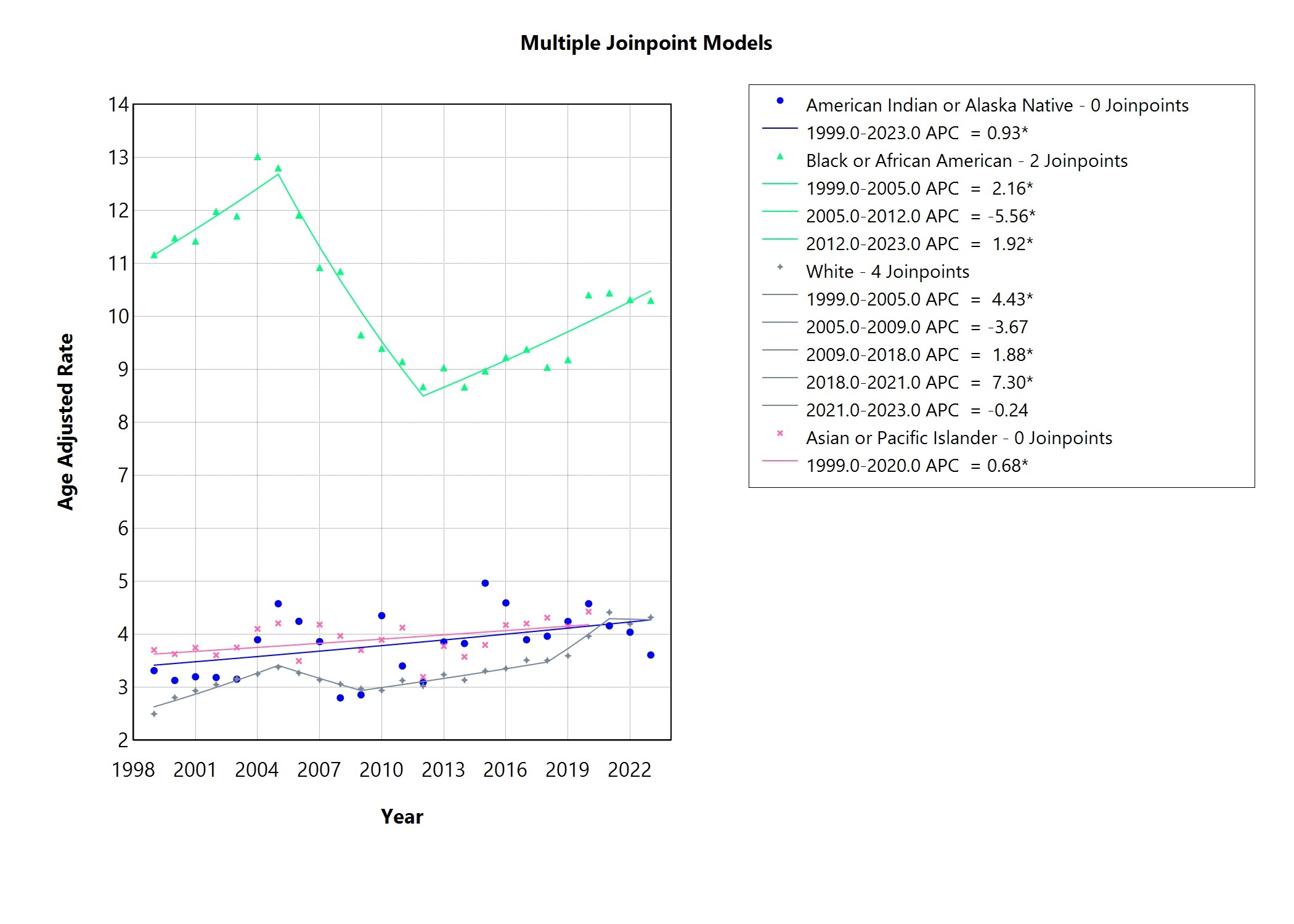
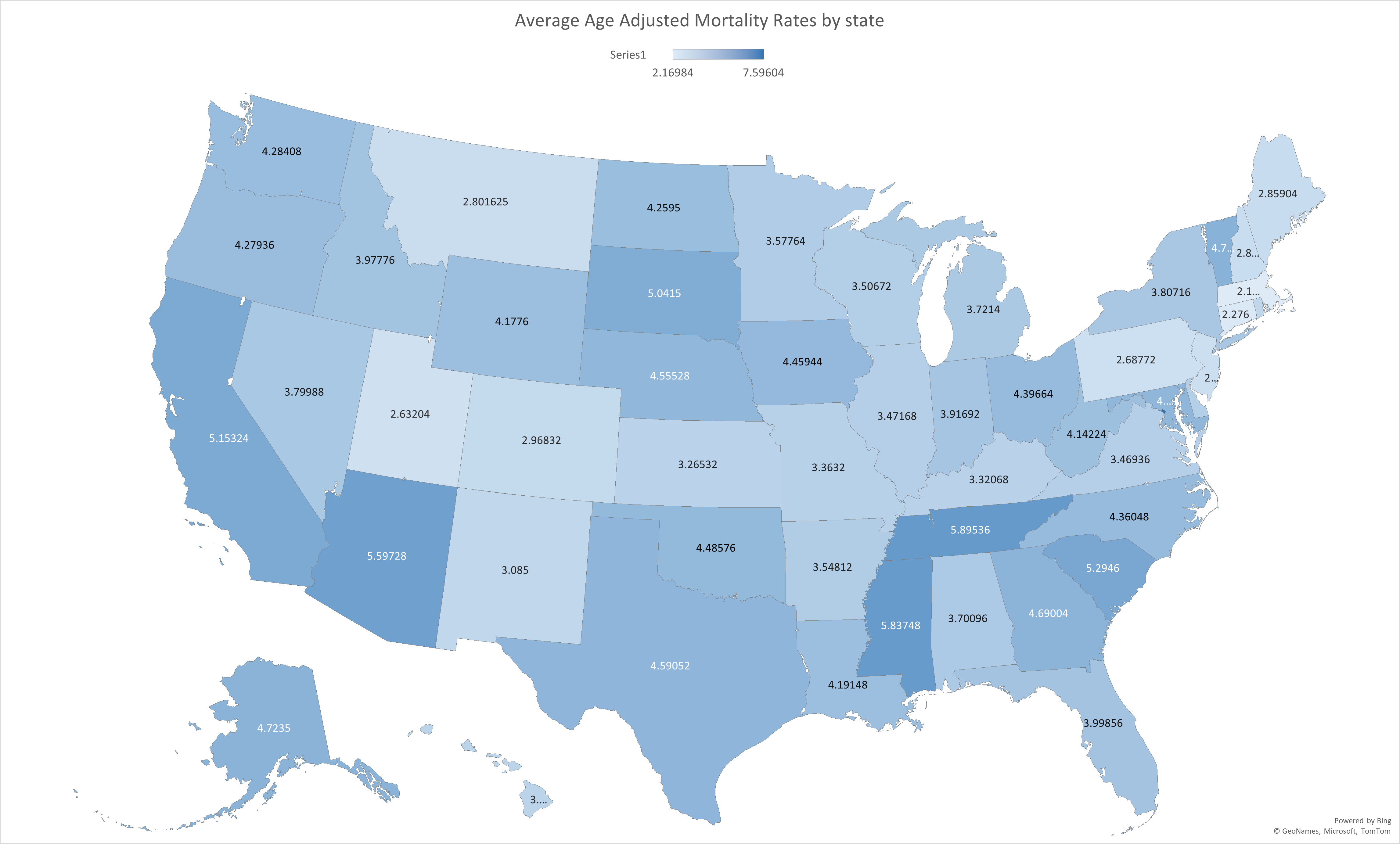
Abstract Body: Background: Hypertension is a major risk factor for end-organ damage, including kidney damage. It is the second leading cause of end-stage renal disease (ESRD) and contributes significantly to morbidity and mortality. This study examined 25-year mortality trends and disparities in hypertensive renal disease in the United States. Methods: We analyzed death data from the Centers for Disease Control and Prevention - Wide-ranging Online Data for Epidemiology Research (CDC - WONDER) database from 1999 to 2023 using ICD-10 codes for hypertensive renal disease with and without renal failure (I12, I12.0, I12.9). Age-adjusted mortality rates (AAMRs) per 100,000 were calculated and stratified by year, sex, race, ethnicity, and region. Joinpoint regression was used to assess trends via average annual percent change (AAPC), and Microsoft Excel was used for other statistical testing, with p < 0.05 considered significant. Results: From 1999 to 2023, hypertensive renal disease caused 274,667 deaths among individuals aged ≥15 years. AAMR rose from 3.3 to 4.91 (AAPC = 1.51%, 95% CI: 0.53–2.50; p = 0.0023). Men had a higher mean AAMR than women (4.48 vs. 3.69; p < 0.001), with a 22% higher mortality in cases with renal failure (p < 0.0001), but no significant sex difference was found in cases without renal failure (p = 0.36). Significant differences were found across racial groups (F(3, 93) = 452.73, p < 0.0001), with Black individuals having the highest mean AAMR (10.37) versus 3.33 - 3.90 in other groups, and this disparity remained consistent regardless of renal failure status. Hispanics had 15% higher AAMRs than non-Hispanics (4.55 vs. 3.97; p < 0.001), though subgroup analysis by renal failure status was limited due to data suppression. Regionally, the West had the highest overall AAMR (4.59), but the three states with the highest rates were in the South: Washington D.C. (7.6), Tennessee (5.9), and Mississippi (5.83). Conclusion: Hypertensive renal disease mortality has significantly increased over the past 25 years, with persistent disparities across race, ethnicity, sex, and region. African American and Hispanic males are disproportionately affected, with African Americans experiencing higher mortality regardless of renal failure status. These findings underscore the urgent need for equitable interventions and efforts to address structural barriers in order to reduce disparities and improve outcomes.
Nyongbella, Joiven
(
Wayne State University
, Rochester Hills , Michigan , United States )
Pineiro De Jesus, Pedro
(
Wayne State University
, Rochester Hills , Michigan , United States )
Lavu, Vamsi Krishna
(
Wayne State University
, Rochester Hills , Michigan , United States )
Aldaoud, Nour
(
Wayne State University
, Rochester Hills , Michigan , United States )
Mohammed Ali, Mohammed
(
Wayne State University
, Rochester Hills , Michigan , United States )
Kotak, Kopal
(
Wayne State University
, Rochester Hills , Michigan , United States )
Saleemi, Aman
(
Wayne State University
, Rochester Hills , Michigan , United States )
Gifford, Kyle
(
Wayne State University
, Rochester Hills , Michigan , United States )
Ajaero, Emecheta
(
Wayne State University
, Rochester Hills , Michigan , United States )
Ebene Mbende, Romain
(
University of Douala
, Douala , Cameroon )
Lattupalli, Ria
(
Troy High School
, Troy , Michigan , United States )
Kulairi, Zain
(
Wayne State University
, Rochester Hills , Michigan , United States )
Author Disclosures:
Joiven Nyongbella:DO NOT have relevant financial relationships
| Romain Ebene Mbende:DO NOT have relevant financial relationships
| Ria Lattupalli:DO NOT have relevant financial relationships
| Zain Kulairi:DO NOT have relevant financial relationships
| Pedro Pineiro De Jesus:DO NOT have relevant financial relationships
| Vamsi Krishna Lavu:DO NOT have relevant financial relationships
| Nour Aldaoud:DO NOT have relevant financial relationships
| Mohammed Mohammed Ali:DO NOT have relevant financial relationships
| Kopal Kotak:DO NOT have relevant financial relationships
| Aman Saleemi:No Answer
| Kyle Gifford:DO NOT have relevant financial relationships
| Emecheta Ajaero:No Answer