Health-Related Social Needs and Hypertension Awareness, Treatment, and Control among Community-Dwelling Black Men
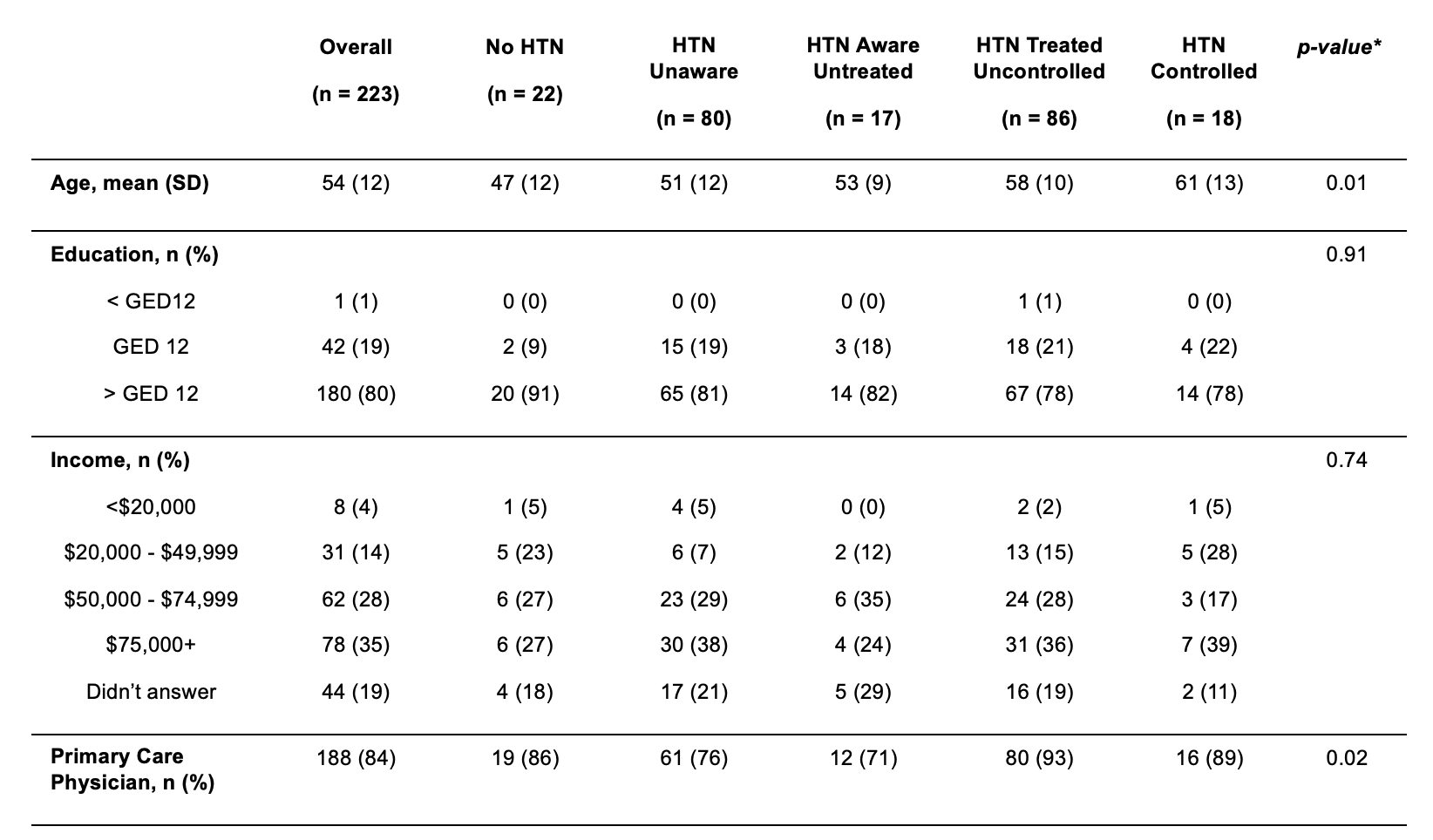
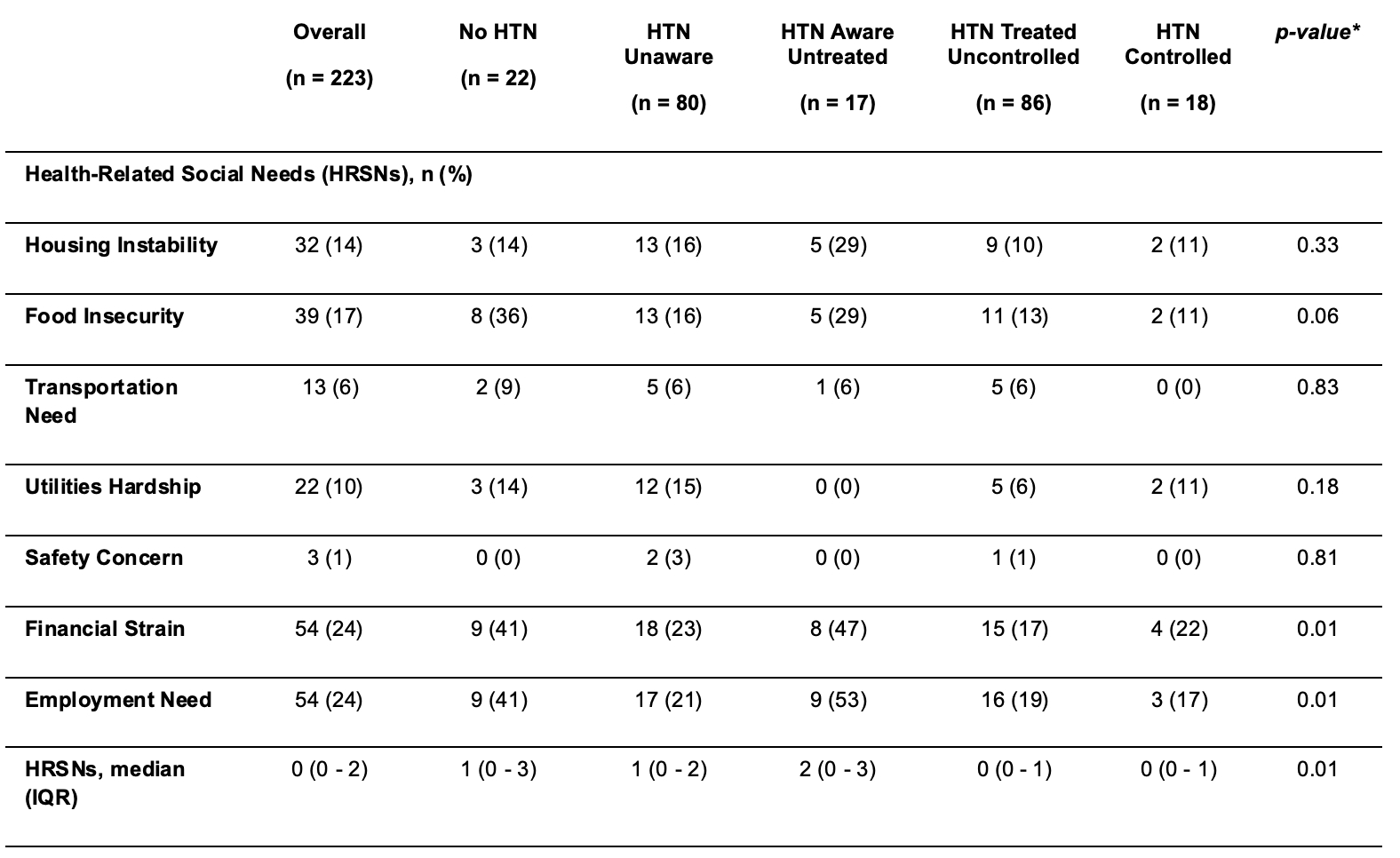
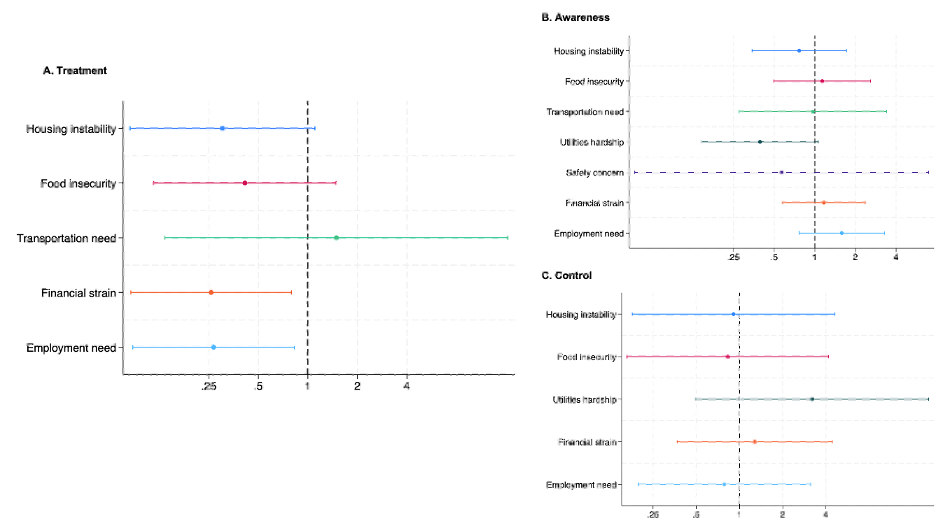
Abstract Body: Non-Hispanic Black men have the highest hypertension (HTN) prevalence and the lowest awareness, treatment, and control in the U.S. Health-related social needs (HRSNs) refer to social and economic conditions that affect health at the individual level. Unmet HRSNs disproportionately affect Black men and worsen care disparities. We evaluated associations between unmet HRSNs and HTN awareness, treatment, and control among community-dwelling Black men in a major Midwestern city. We conducted a cross-sectional baseline analysis of the Black Impact study, a 24-week randomized community lifestyle trial of Black men with low–to–moderate cardiovascular health in central Ohio. HTN was defined as systolic/diastolic blood pressure ≥130/80 mm Hg, current antihypertensive medication use, or self-reported diagnosis. Outcomes were awareness (self-reported diagnosis), treatment (antihypertensive medication use), and control among those treated (blood pressure <130/80 mm Hg). HRSNs were assessed with the Accountable Health Communities screening tool (housing, food, transportation, utilities, safety, financial strain, employment). Each domain was handled as unmet (yes/no); total HRSNs were summed (0–7). Logistic regression estimated the odds of awareness, treatment, and control by domain and per 1-unit increase in the HRSN count. Model 1 adjusted for age; Model 2 for age and primary care physician (PCP). We analyzed 223 Black men, mean (SD) age was 54 (12) years (Table 1); 84% had a PCP and 19% had ≥1 HRSN (Table 2). Distribution across the cascade was: normotensive, 10%; unaware, 36%; aware–untreated, 8%; treated–uncontrolled, 38%; treated–controlled, 8%. In age-adjusted models, housing instability (OR 0.26, 95% CI: 0.08, 0.91), financial strain (OR 0.25, 95% CI: 0.08, 0.73), and employment need (OR 0.21, 95% CI: 0.07, 0.61) were associated with decreased odds of being treated, with only housing instability being attenuated in further adjustment. For the HRSN count, each additional unmet need was associated with a 46% and 32% decrease in the odds of being treated in model 1 and model 2, respectively (both p<0.05). Associations with awareness were modest and not significant (Figure). No HRSN domain was associated with HTN control among treated participants. Screening and addressing HRSNs—especially financial strain and employment—within community and clinical programs may improve treatment uptake and advance progression along the hypertension care cascade for Black men.
Baylon-valdez, Victor
(
The Ohio State University
, Columbus , Ohio , United States )
Williams, Amaris
(
The Ohio State University
, Columbus , Ohio , United States )
Nolan, Timiya
(
University of Alabama at Birmingham
, Birmingham , Alabama , United States )
Lartey, Kwame
(
The Ohio State University
, Columbus , Ohio , United States )
Ojembe, Nnanna
(
The Ohio State University
, Columbus , Ohio , United States )
Matambo, Sean
(
The Ohio State University
, Columbus , Ohio , United States )
Wilson, Amani
(
The Ohio State University
, Columbus , Ohio , United States )
Davis, Loletia
(
The Ohio State University
, Columbus , Ohio , United States )
Gregory, John
(
5The African American Male Wellness Agency
, Columbus , Ohio , United States )
Donneyong, Macarius
(
The Ohio State University
, Columbus , Ohio , United States )
Joseph, Joshua
(
The Ohio State University
, Columbus , Ohio , United States )
Ali Muhammad Faizan, Khan Muhammad, Sharif Aleena, Hossain Mohammad, Ahmad Husnain, Eltawansy Sherif, Faizan Muhammad, Ahmed Ashraf, Abdul Malik Mohammad Hamza Bin, Pahwani Ritesh, Patel Rahul, Mehdi Hassan
Lartey Kwame, Matambo Sean, Smith Shabrya, Sivakumar Sadhana, Davis Loletia, Gillespie Shannon, Nolan Timiya, Gregory John, Joseph Joshua, Ojembe Nnanna, Wilson Amani, Williams Amaris, Brock Guy, Zhao Songzhu, Grant Jeremy, Greer Darreon, Griffin Madison