Sex Disparities in Accuracy of Physician-Reported Versus Computed CHA2DS2-VASc Scores in the Get With The Guidelines–AFIB Registry
Abstract Body: Introduction The CHA2DS2-VASc score is a widely used tool for stroke risk stratification in atrial fibrillation/ flutter (AF/AFL). Inaccurate scores can lead to inappropriate treatment. Data are limited on whether reporting accuracy differs by patient sex.
Hypothesis We hypothesized that inaccurate physician-reported CHA2DS2-VASc scores disproportionally affect younger females with AF/AFL, in whom underreporting may result in missed opportunities for stroke prevention.
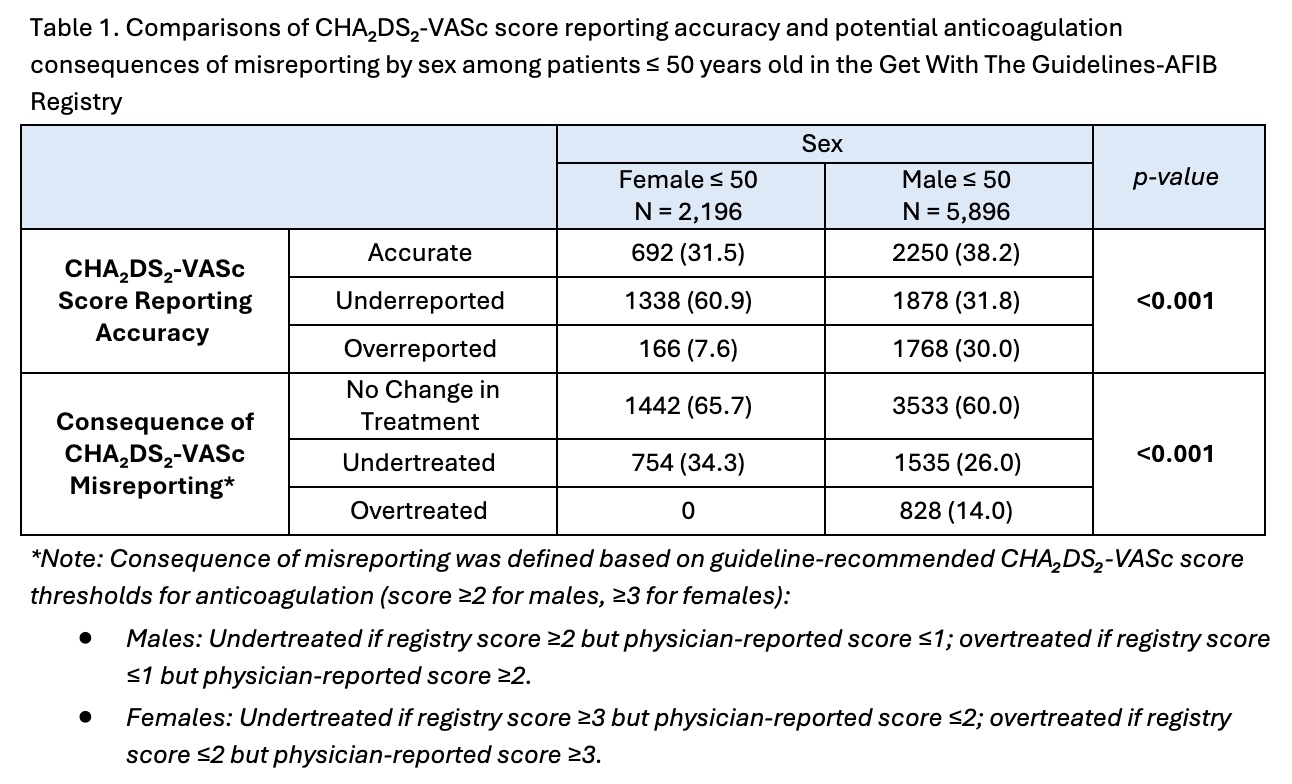
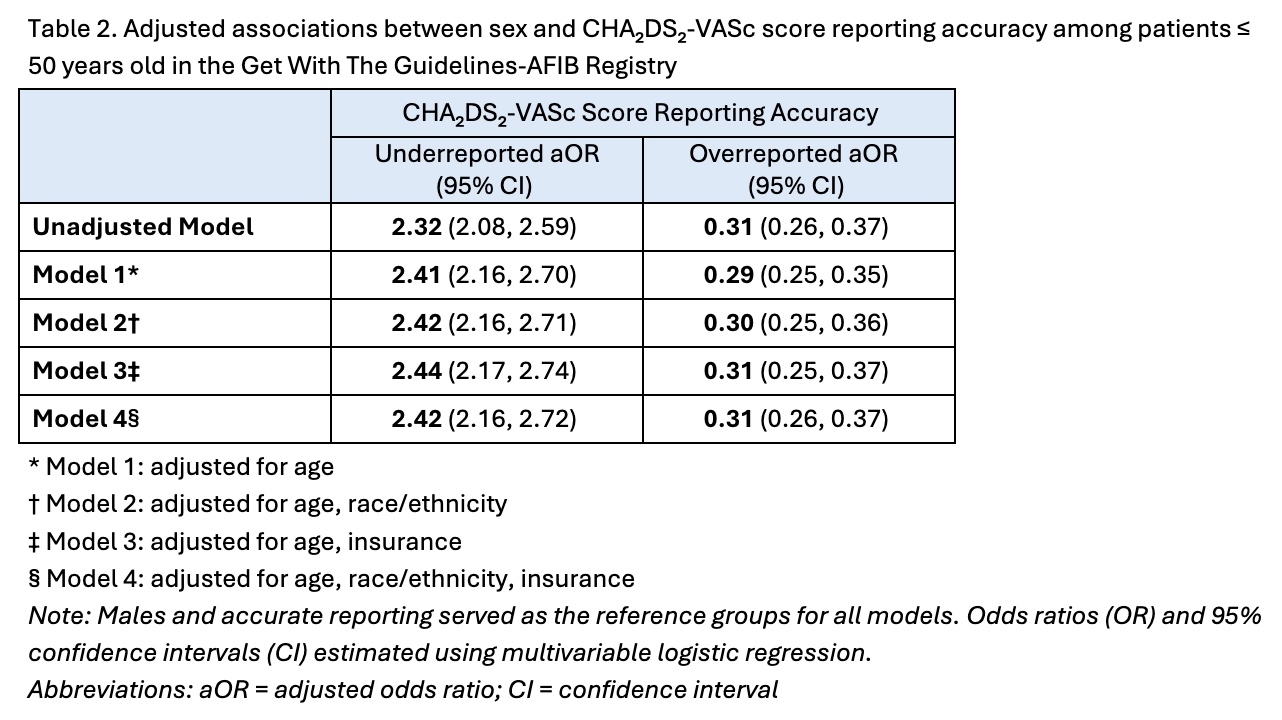
Methods We included reproductive-age patients (≤50 years) with AF/AFL from the Get With The Guidelines–AFIB registry from May 2013 to March 2024. Physician-reported CHA2DS2-VASc scores were compared with registry-computed scores and categorized as accurate, underreported, or overreported. Misreporting consequences (no change, undertreatment, or overtreatment) were based on guideline-recommended anticoagulation thresholds. Associations between sex and reporting accuracy were assessed using chi-square tests and multivariable logistic regression to estimate odds ratios (ORs), which were adjusted for age, race/ethnicity, and insurance.
Results This analysis included 8,092 patients with 27.1% female and mean ages 42.5 ± 7.0 (females) and 42.0 ± 7.4 years (males). Physician-reported CHA2DS2-VASc scores were 1.35 ± 0.61 for females and 1.27 ± 0.52 for males. Compared to registry scores, females were significantly more likely to have underreported physician scores (60.9% vs 31.8%), whereas males were more often overreported (30.0% vs 7.6%; p<0.001, Table 1). Unadjusted regression analyses confirmed that females had over twice the odds of underreporting (OR 2.32, 95% CI 2.08–2.59) and 69% lower odds of overreporting (OR 0.31, 95% CI 0.26–0.37) versus males (Table 2). These findings persisted after adjustment for age, race/ethnicity, and insurance. Potential consequences of misreporting also differed by sex. Females were more likely to be undertreated (34.3% vs 26.0%, p<0.001), while males were more likely to be overtreated with anticoagulation based on physician-reported scores (14.0% vs 0.0%, p<0.001).
Conclusion Among reproductive-age patients with AF/AFL, physician-reported CHA2DS2-VASc scores were less accurate for females than males, primarily due to underreporting. These sex-based discrepancies may contribute to undertreatment and missed opportunities for stroke prevention in younger women. Efforts to improve accuracy in scoring are needed to ensure equitable preventative care in AF/AFL.
Barnes, Jenna
(
UMass Chan Medical School
, Worcester , Massachusetts , United States )
Denoncourt, Cailey
(
UMass Chan Medical School
, Worcester , Massachusetts , United States )
Wang, Ziyue
(
UMass Chan Medical School
, Worcester , Massachusetts , United States )
Wilkie, Gianna
(
UMass Chan Medical School
, Worcester , Massachusetts , United States )
Alhuarrat, Majd Al Deen
(
UMass Chan Medical School
, Worcester , Massachusetts , United States )
Kiani, Soroosh
(
UMass Chan Medical School
, Worcester , Massachusetts , United States )
Kovell, Lara
(
UMass Chan Medical School
, Worcester , Massachusetts , United States )