Smoking Cessation or Reduction After Myocardial Infarction and Subsequent Risk of Cardiovascular Events
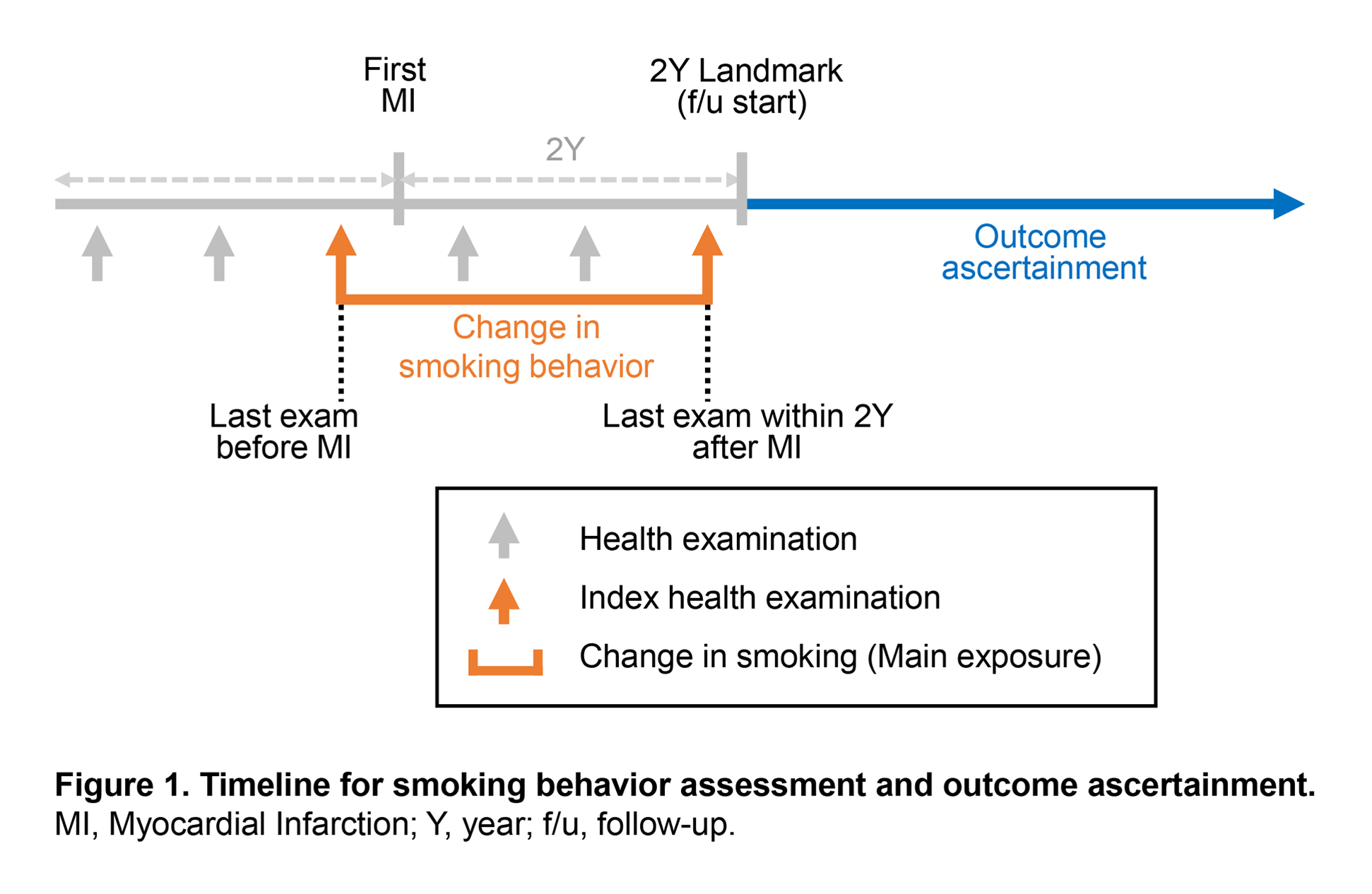
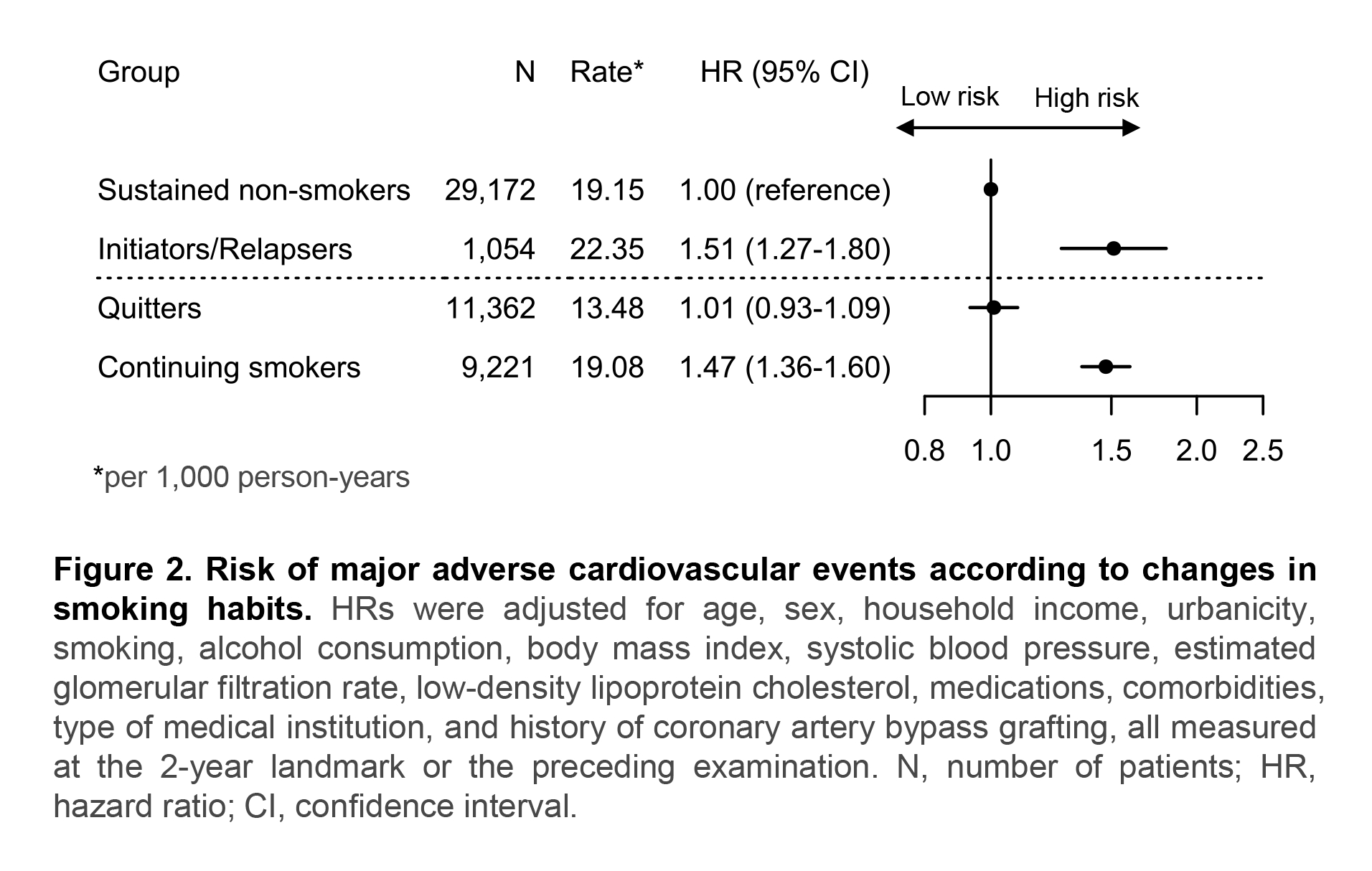
Abstract Body: Introduction: While smoking is a major risk factor for cardiovascular disease, data are scarce regarding the outcomes of smoking cessation and reduction after myocardial infarction (MI) among those who smoked. We hypothesized that smoking cessation but not reduction was associated with a lower risk of major adverse cardiovascular events (MACE) after first MI. Methods: Using the Korean National Health Insurance Service database, we included adults aged ≥19 years who experienced first MI between 2009 and 2019 and had health examination records before MI and during the 2-year landmark period after the MI (Figure 1). Smoking status and amount (cigarettes/day) were self-reported at each examination. Based on changes between pre- and post-MI examinations, participants were categorized as sustained non-smokers, initiators/relapsers, quitters, or continuing smokers. Among pre-MI smokers, participants were further categorized based on post-MI smoking amount as quitters, reducers (≥50% decrease in cigarettes/day), or non-reducers. The primary outcome was first occurrence of MACE (composite of cardiovascular death, stroke, or recurrent MI). Secondary outcomes included all-cause death, first occurrence of each component of MACE, and total (first and subsequent) occurrence (i.e., recurrent event analysis) of MACE. Results: Among 50,809 adults included, mean±SD age was 63.5±11.1 years at landmark, and 19.2% were women. After first MI, 55.2% of pre-MI smokers quit and 11.2% reduced smoking by ≥50%, whereas 3.5% of pre-MI non-smokers initiated or relapsed into smoking. Over a median follow-up of 5.5 years (IQR, 3.5-7.5 years) from the 2-year landmark, 5,033 primary outcome events occurred. Compared with sustained non-smokers, multivariable-adjusted HR (95% CI) for MACE was 1.51 (1.27-1.80) for initiators/relapsers, 1.01 (0.93-1.09) for quitters, and 1.47 (1.36-1.60) for continuing smokers (Figure 2). Among pre-MI smokers, quitting was associated with a lower risk of MACE (HR, 0.69; 95% CI, 0.62-0.76), whereas reducing by ≥50% was not (HR, 0.98; 95% CI, 0.85-1.14), compared with continued smoking without reduction (Figure 3). Smoking reduction was not associated with lower risk even when stratified by pre-MI smoking amount. Results were consistent for secondary and recurrent outcomes. Conclusions: Smoking cessation after MI was associated with a substantially lower risk of subsequent cardiovascular events, whereas smoking reduction without cessation did not confer lower risk.
Shin, Sojung
(
Yonsei University College of Medicine
, Seoul , Korea (the Republic of) )
Khil, Jaewon
(
Yonsei University College of Medicine
, Seoul , Korea (the Republic of) )
Cheon, Dae Young
(
Hallym University Dongtan Sacred Heart Hospital
, Hwaseong , Korea (the Republic of) )
Lee, Jaeyong
(
Yonsei University College of Medicine
, Seoul , Korea (the Republic of) )
Ha, Kyoung Hwa
(
Yonsei University College of Medicine
, Seoul , Korea (the Republic of) )
Lee, Hyeok-hee
(
Beth Israel Deaconess Medical Center, Harvard Medical School
, Boston , Massachusetts , United States )
Kim, Hyeon Chang
(
Yonsei University College of Medicine
, Seoul , Korea (the Republic of) )
Lee, Hokyou
(
Yonsei University College of Medicine
, Seoul , Korea (the Republic of) )