Intravascular ultrasound and hemodynamics in stenotic lesions of arteriovenous fistulas or grafts in patients on hemodialysis
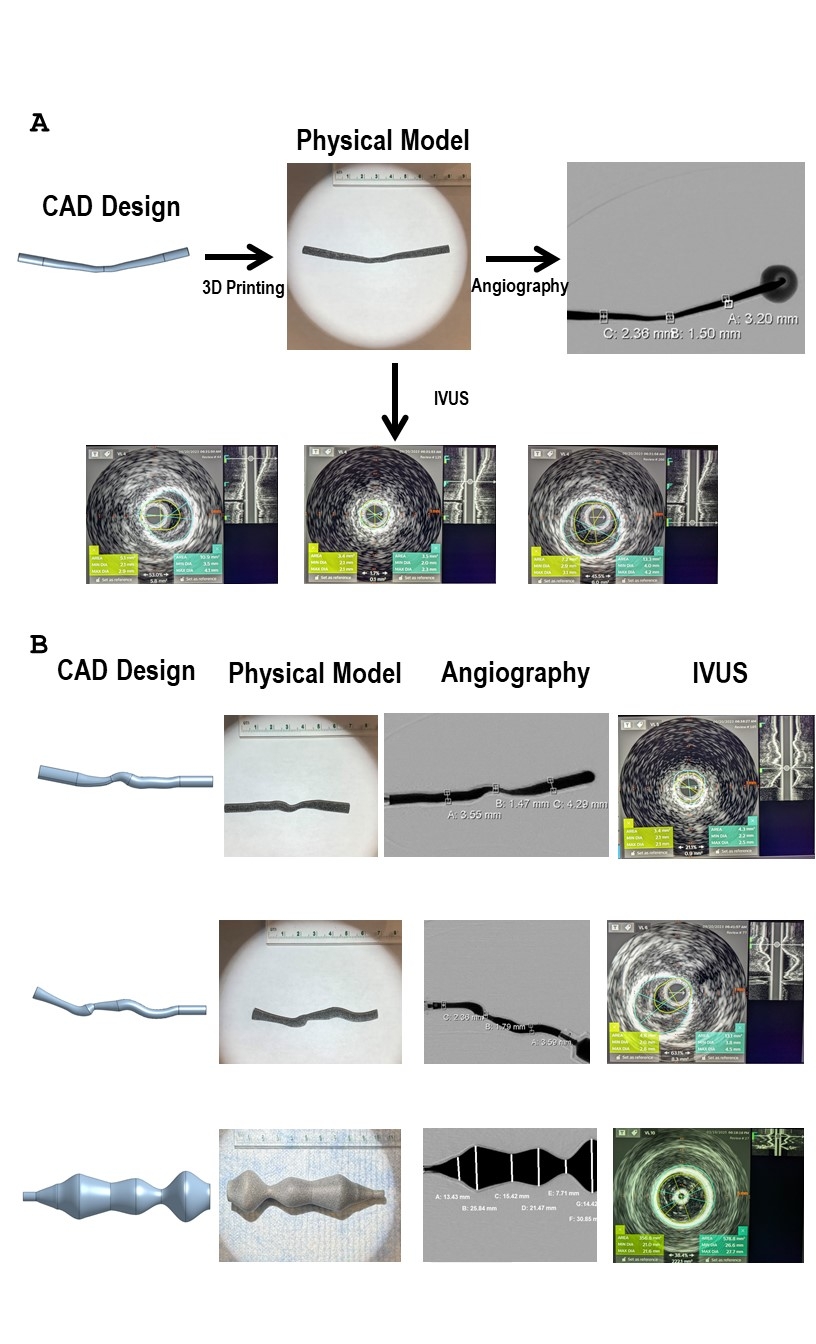
Abstract Body: Background Chronic kidney disease (CKD) is a major public health crisis. In the US, one out of seven people has CKD. Of these, over 815,000 people have end-stage kidney disease (ESKD). Approximately 550,000 people undergo hemodialysis treatment in the US. Arteriovenous (AV) vascular accesses, such as arteriovenous fistulas (AVFs) or arteriovenous grafts (AVGs), are required for hemodialysis. Conventional angiography remains the standard diagnostic modality for access dysfunction, but its geometric accuracy is limited. Intravascular ultrasound (IVUS) offers superior lesion detection, yet its accuracy remains uncertain. Using three-dimensional (3D) printed vascular conduits as reference standards, we assessed the accuracy of IVUS versus angiography, hypothesizing that complex conduit geometry, quantified by Gaussian curvature, would exacerbate angiographic error. Methods Clinically relevant AV access geometries were modeled with computer-aided design (CAD) and fabricated using 3D printing. Lumen diameters were measured by contrast angiography and IVUS, and then compared against CAD dimensions. Conduit geometry was characterized using finite element–based Gaussian curvature mapping. Statistical analyses examined measurement errors, their relationship to geometric complexity and differences across imaging modalities. Results IVUS demonstrated significantly lower measurement error, particularly in stenotic segments with greater than 50% luminal narrowing. This high-grade stenosis frequently coincided with regions of high positive or negative Gaussian curvature, reflecting the complex geometry of the conduit. In such regions, angiography consistently underestimated lumen diameter, with error magnitude increasing in tortuous segments. IVUS measurements closely approximated CAD ground truth, retaining accuracy even in severe stenosis. For mild stenosis (<50%) and aneurysmal dilatations, both modalities performed comparably. Conclusion Geometric complexity directly contributes to modality-specific error. Angiography systematically underestimates lumen dimensions in complex, stenotic regions, while IVUS preserves accuracy. These findings establish IVUS as the more reliable modality for evaluating AV access dysfunction and support its integration into routine practice for guiding intervention in AV access stenosis.
Lotfollahzadeh, Saran
(
Boston University School of Medicin
, Boston , Massachusetts , United States )
Siracuse, Jeffrey
(
Boston University
, Chestnut Hill , Massachusetts , United States )
Farber, Alik
(
Boston Medical Center
, Boston , Massachusetts , United States )
Kolachalama, Vijaya
(
BU SCHOOL OF MEDICINE
, Boston , Massachusetts , United States )
Ganguli, Suvranu
(
Boston University School of Medicin
, Boston , Massachusetts , United States )
Chitalia, Vipul
(
Boston University School of Medicin
, Boston , Massachusetts , United States )