Evaluating the Implications of PREVENT Risk Estimates for Non-Cardiovascular Outcomes: The Atherosclerosis Risk in Communities (ARIC) Study
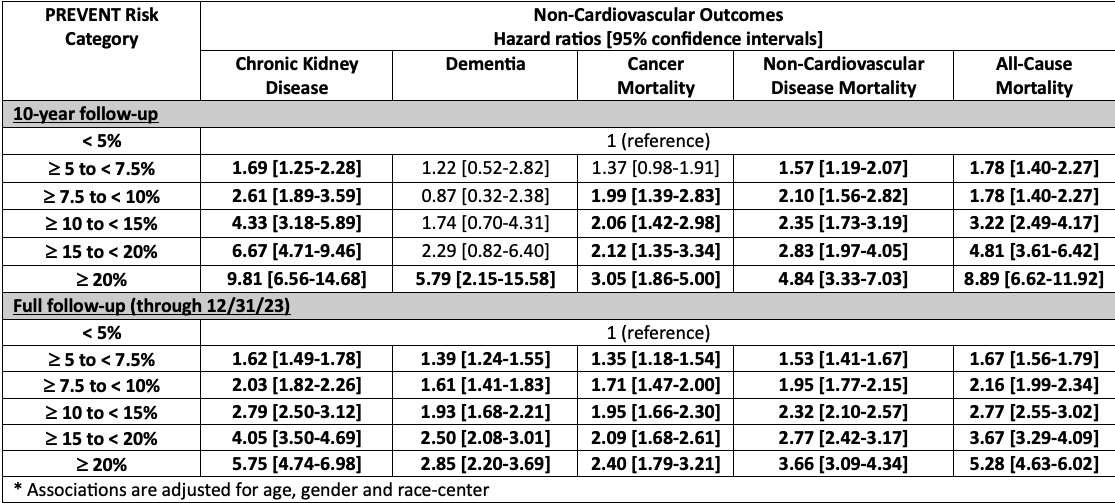
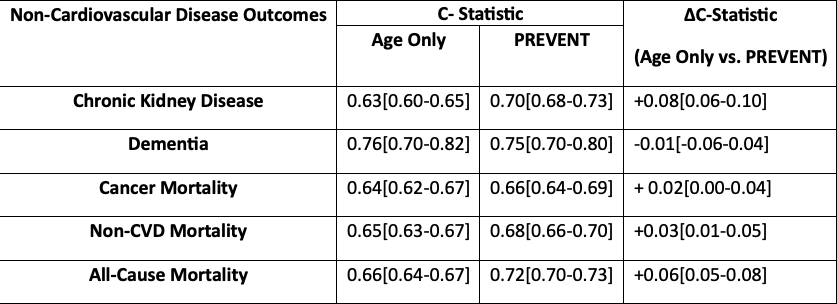
Abstract Body: Introduction: In response to the growing burden of poor cardiovascular-kidney-metabolic (CKM) health, the PREVENT equations were developed to incorporate emerging risk factors and improve contemporary cardiovascular risk prediction. Poor CKM health has multiorgan consequences that extend beyond the cardiovascular system, yet the implications of PREVENT risk estimates for non-cardiovascular disease (non-CVD) outcomes are presently unclear. Methods: We performed a prospective analysis of 11,132 participants at ARIC Visit 2 (1990–1992) without baseline CVD. PREVENT-CVD 10-year risk estimates were calculated using Visit 2 data and categorized as <5%, 5 to <7.5%; 7.5 to <10%; 10 to <15%; 15 to <20%; and ≥20%. Multivariate cause-specific Cox regression was performed to estimate associations of higher PREVENT-CVD risk categories with the non-CVD outcomes of incident chronic kidney disease (CKD), dementia, cancer mortality, non-CVD mortality and all-cause mortality over 10 years and through 12/31/23. For those who had events, median time-to-event by quantile regression from age 60 was calculated for each PREVENT category. For each outcome, 10-year risk discrimination was assessed by calculating Harrell’s C-statistics. Results: Within the study population (mean age 57 years; 57% women; 25% Black adults), 4,173 participants developed CKD, 2,802 developed dementia, 1,943 died from cancer, 5,069 died from non-CVD causes, and 7,232 died from any cause. There was a dose–response increase in the hazards of each non-CVD outcome with higher PREVENT-CVD risk categories (Table 1). At 10 years, PREVENT-CVD ≥20% (versus <5%) was associated with HRs of 9.81 (95% CI 6.56-14.68) for incident CKD, 5.79 (95% CI 2.15-15.58) for dementia, 3.08 (95% CI 1.86-5.00) for cancer mortality, 4.84 (95% CI 3.33-7.03) for non-CVD mortality and 8.89 (95% CI 6.62-11.92) for all-cause mortality. Significant associations were also seen at full follow-up. Higher PREVENT categories were associated with progressively shorter time-to-event for all non-CVD outcomes (Figure), with non-CVD and all-cause mortality occurring ~11 and 13 years earlier with PREVENT-CVD ≥20% versus <5%. PREVENT improved 10-year risk discrimination beyond age alone for most non-CVD outcomes (Table 2). Conclusion: Higher PREVENT-CVD scores suggest greater risk and shorter time to event for multiple non-CVD outcomes. Employing strategies to enhance CKM health likely has implications for global clinical outcomes.
Grant, Jelani
(
Johns Hopkins Hospital
, Parkville , Maryland , United States )
Zhang, Sui
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Khan, Sadiya
(
Northwestern University
, Chicago , Illinois , United States )
Wallace, Amelia
(
JH Bloomberg Sch. of Public Health
, Baltimore , Maryland , United States )
Troy, Aaron
(
Johns Hopkins Hospital
, Pikesville , Maryland , United States )
Echouffo, Justin
(
Johns Hopkins Hospital
, Baltimore , Maryland , United States )
Nambi, Vijay
(
Baylor College of Medicine
, Sugar Land , Texas , United States )
Blumenthal, Roger
(
Roger Blumenthal
, Baltimore , Maryland , United States )
Matsushita, Kunihiro
(
JOHNS HOPKINS UNIVERSITY
, Baltimore , Maryland , United States )
Ballantyne, Christie
(
BAYLOR COLLEGE MEDICINE
, Houston , Texas , United States )
Coresh, Joe
(
JOHNS HOPKINS SPH WELCH CENTER
, Baltimore , Maryland , United States )
Ndumele, Chiadi
(
JOHNS HOPKINS HOSPITAL
, Silver Spring , Maryland , United States )