Incidentally Detected Coronary Calcium and the Burden and Severity of Cardiovascular-Kidney Metabolic Risk Factors
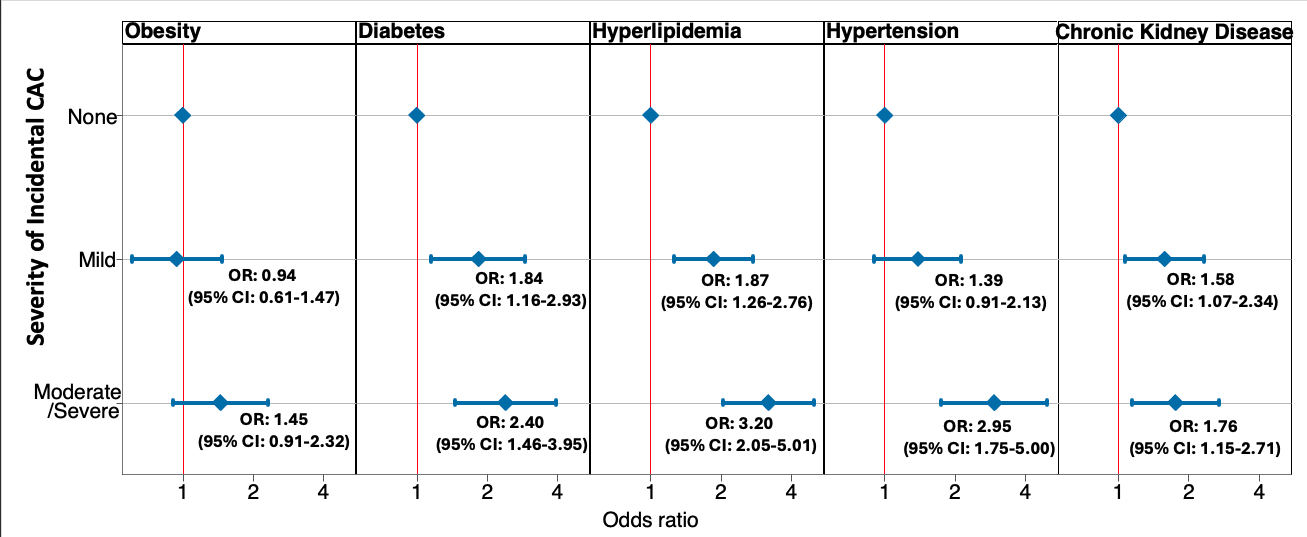
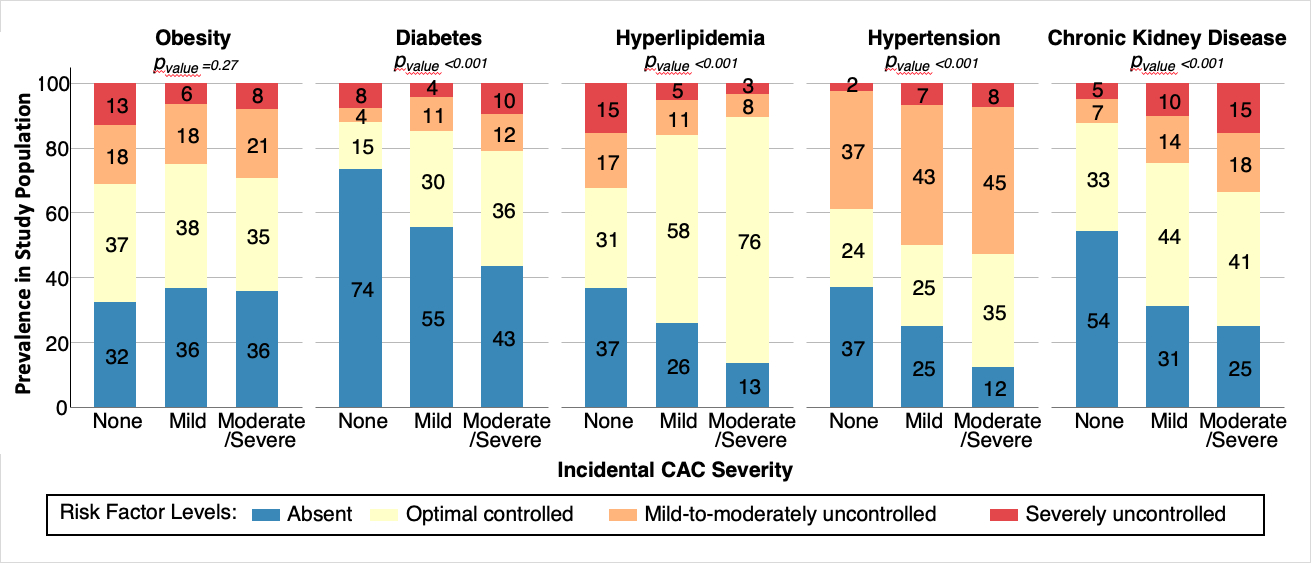
Abstract Body: Introduction: Coronary artery calcium (CAC) incidentally found on non-EKG-gated cardiac chest CT scans identifies individuals at elevated ASCVD risk, providing an opportunity for intensified preventive pharmacotherapy. While lipid lowering therapy for those with elevated CAC is a focus of clinical guidelines, it is unclear the extent to which other cardiovascular-kidney-metabolic (CKM) risk factors may represent preventive targets. Methods: We conducted a cross-sectional analysis of 760 adults who underwent non-ECG-gated, non-cardiac chest CTs at the University of Miami between 2019–2021. CAC severity was categorized visually as none, mild, or moderate-to-severe. Across levels of incidental CAC severity, we used logistic regression to estimate the odds of the CKM risk factors of obesity, diabetes, HTN, hyperlipidemia and CKD. We also assessed risk factor control/severity (absent, controlled, mild/moderate, severe) across CAC levels. We used ordinal logistic regression to assess the odds of worse CKM risk factor severity/control for those with mild and moderate-to-severe CAC relative to those with no CAC. Results: Mean age was 63 years, with 52% women, and 54% Hispanic adults. CAC distribution was none (40.7%), mild (27.2%), and moderate-to-severe (32.1%). Across increasing severity of incidental CAC, the odds of prevalent risk factors increased for all CKM risk factors except obesity (Figure 1). The prevalence of more uncontrolled/severe risk factors increased progressively from no CAC to moderate-to-severe CAC for diabetes (11 vs 24%), HTN (39 vs 54%) and CKD (12 vs 41%) (Figure 2). Conversely, less uncontrolled hyperlipidemia was seen with higher CAC (32% with no CAC vs 10% with moderate-to-severe CAC), corresponding to more moderate-high intensity statin use with higher CAC (22% with no CAC vs 62% with moderate-to-severe CAC). Those with higher incidental CAC had higher odds of worse risk factor severity/control for diabetes, HTN and CKD (ORs 3.46, 1.50 and 1.82, respectively, for those with moderate-to-severe versus no incidental CAC), with no associations for obesity or hyperlipidemia (Table). Conclusion: The prevalence and severity of CKM risk factors are associated with more severe incidental CAC. While lipid control has been a clinical focus for individuals with incidental CAC, addressing diabetes, HTN and CKD with proven cardioprotective therapies and lifestyle improvements holds promise for enhancing preventive care for this high-risk population.
Pan, Abigail
(
Johns Hopkins University School of Medicine
, Baltimore , Maryland , United States )
Zhang, Sui
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Martin, Seth
(
Johns Hopkins School of Medicine
, Baltimore , Maryland , United States )
Pagidipati, Neha
(
Duke University School of Medicine
, Durham , North Carolina , United States )
Blumenthal, Roger
(
Johns Hopkins University School of Medicine
, Baltimore , Maryland , United States )
Orringer, Carl
(
Naples Comprehensive Health System
, Naples , Florida , United States )
Rangaswami, Janani
(
The George Washington University School of Medicine and Health Sciences
, Washington D.C. , District of Columbia , United States )
Ndumele, Chiadi
(
Johns Hopkins University School of Medicine
, Baltimore , Maryland , United States )
Grant, Jelani
(
Johns Hopkins University School of Medicine
, Baltimore , Maryland , United States )