Extra-Coronary Calcification and Risk of Incident Cardiovascular Disease in Adults 75 and Older: The Atherosclerosis Risk in Communities (ARIC) Study
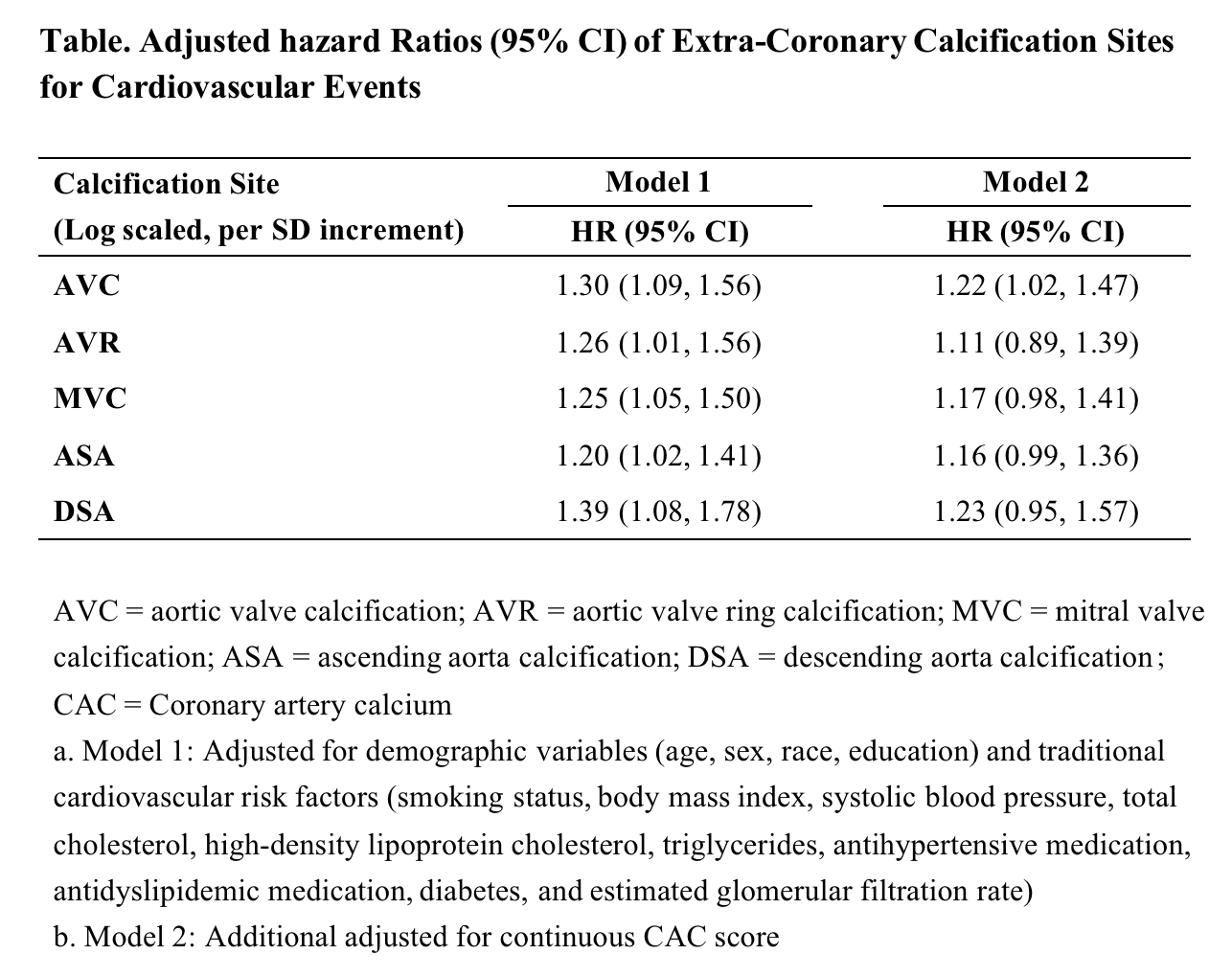
Abstract Body: Background: The coronary artery calcium (CAC) score is one of the most potent predictors of cardiovascular disease (CVD). During a CAC scan, extra-coronary calcification (ECC) can be simultaneously measured, but the independent prognostic value is unknown in adults aged 75 and older. Methods: We studied 1,831 ARIC participants at visit 7 (mean age 80.4 [SD 4.2] years, 62% female, 20% black) without prevalent CVD. We quantified ECC (Agatston score) at five specific sites: aortic valve calcification (AVC), aortic valve ring calcification (AVR), mitral valve calcification (MVC), ascending aorta calcification (ASA), and descending aorta calcification (DSA). We ran multivariable Cox models with total CVD events (composite of adjudicated myocardial infarction, stroke, and heart failure) as the outcome. Results: Over a mean follow-up of 2.6 years, 113 incident CVD events occurred. The prevalence of ECC>0 varied by site: AVC (45%), ARC (86%), MVC (47%), ASA (25%), and DSA (89%). After adjusting for traditional CVD risk factors (Model 1 in Table), prevalence of each ECC was associated with incident CVD events (e.g., hazard ratio 1.30, [95%CI 1.09-1.56] for AVC). However, after further adjustment for the CAC score (Model 2 in Table), only AVC remained significant (hazard ratio 1.22 [1.02-1.47]). When adding each ECC into the base model with traditional risk factors and CAC score, AVC, but not other ECCs, significantly improved CVD risk prediction (Δc-statistic 0.014 [95%CI 0.001 to 0.033] from c-statistic of 0.703 to 0.718). Conclusion: Of ECCs measured, AVC was particularly robustly associated with incident CVD and improved CVD prediction beyond CAC score in the 75-and-older population. Our findings suggest the value of quantifying ECC when CAC scan was performed in this population.
Zou, Siyu
(
Johns Hopkins Bloomberg School of Public Health
, Baltimore , Maryland , United States )
Liu, Hairong
(
Johns Hopkins Bloomberg School of Public Health
, Baltimore , Maryland , United States )
Mok, Yejin
(
Johns Hopkins Bloomberg School of Public Health
, Baltimore , Maryland , United States )
Gami, Abhishek
(
Johns Hopkins University School of Medicine
, Baltimore , Maryland , United States )
Chen, Lin Yee
(
UNIVERSITY OF MINNESOTA
, Minneapolis , Minnesota , United States )
Budoff, Matthew
(
LUNDQUIST INSTITUTE
, Torrance , California , United States )
Blaha, Michael
(
JOHNS HOPKINS HOSPITAL
, Baltimore , Maryland , United States )
Matsushita, Kunihiro
(
Johns Hopkins Bloomberg School of Public Health
, Baltimore , Maryland , United States )
Author Disclosures:
Siyu Zou:DO NOT have relevant financial relationships
| Hairong Liu:No Answer
| Yejin Mok:DO NOT have relevant financial relationships
| Abhishek Gami:DO NOT have relevant financial relationships
| Lin Yee Chen:DO NOT have relevant financial relationships
| Matthew Budoff:DO NOT have relevant financial relationships
| Michael Blaha:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Novo Nordisk:Active (exists now)
; Advisor:New Amsterdam:Active (exists now)
; Advisor:Genentech:Active (exists now)
; Advisor:Idorsia:Active (exists now)
; Advisor:Vectura:Active (exists now)
; Advisor:Agepha:Active (exists now)
; Advisor:Boehringer Ingelheim:Active (exists now)
; Advisor:Astra Zeneca:Active (exists now)
; Advisor:Eli Lilly:Active (exists now)
; Advisor:Merck:Active (exists now)
; Advisor:Novartis:Active (exists now)
; Advisor:Bayer:Active (exists now)
; Advisor:Novo Nordisk:Active (exists now)
; Research Funding (PI or named investigator):Bayer:Active (exists now)
| Kunihiro Matsushita:No Answer