Outcomes of Colorectal Cancer Patients with Comorbid Heart Failure: A 22-Year National Analysis
Abstract Body: Background: Colorectal cancer (CRC) is the second leading cause of cancer-related deaths in the United States. Heart failure (HF) is a prevalent comorbidity among CRC patients, contributing to increased postoperative complications, extended hospital stays, and elevated mortality rates. However, national trends and disparities in CRC-related mortality among patients with comorbid HF remain poorly characterized.
Objective: We aimed to evaluate longitudinal trends, demographic differences, and geographic variations in mortality attributed to CRC in patients with HF in the United States.
Methods: A total of 32,204 mortality records from the CDC WONDER database were analyzed for individuals aged >35 years from 1999 to 2020. CRC (ICD-10 codes C18-C20) was identified as the underlying cause of death, with HF (I11.0, I13.0, I13.2, I50) as a contributing cause. Age-adjusted mortality rates (AAMRs) per 1,000,000 were calculated. Joinpoint regression was used to assess temporal trends and annual percent change (APC).
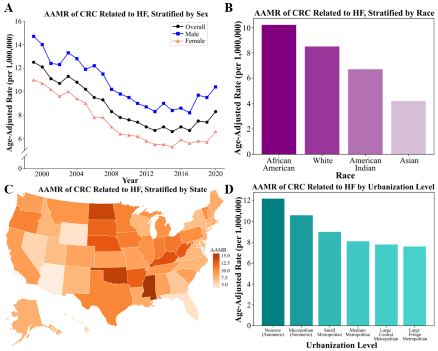
Results:From 1999 to 2015, the AAMR decreased from 12.5 (95% CI, 11.9-13.1) to 6.6 (95% CI, 6.2-6.9), with an APC of -4.2% (p<0.01). However, from 2015 to 2020, the AAMR significantly increased to 8.3 (95% CI, 7.9-8.7), with an APC of 5.0% (p<0.01). Cumulative AAMRs were higher in males (10.4 [95% CI, 10.2-10.5]) than females (7.2 [95% CI, 7.1-7.3]). Among racial groups, African Americans exhibited the highest AAMR (10.2 [95% CI, 9.9-10.6]), followed by White individuals (8.5 [95% CI, 8.4-8.6]), American Indians (6.7 [95% CI, 5.6-7.8]), and Asians (4.2 [95% CI, 3.8-4.5]). Rural noncore areas had higher AAMRs than large central metropolitan areas (12.2 [95% CI, 11.8-12.6] vs. 7.8 [95% CI, 7.7-8.0]). Geographically, the Midwest region had the highest AAMR (9.9 [95% CI, 9.7-10.1]), followed by the South (8.3 [95% CI, 8.1-8.4]), West (8.1 [95% CI, 7.9-8.3]), and Northeast (7.9 [95% CI, 7.7-8.1]).
Conclusion: While CRC-related mortality with comorbid HF declined from 1999 to 2015, the subsequent rise in AAMR after 2015 displays a concerning shift in mortality trends. Disparities persist across sex, race, and geographic location, highlighting the need for targeted interventions to mitigate these inequities and improve outcomes for high-risk populations.
Ashar, Perisa
(
Duke University
, Durham , North Carolina , United States )
Tamirisa, Ketan
(
Washington University in St. Louis
, St. Louis , Missouri , United States )
Garg, Shriya
(
University of Georgia
, Athens , Georgia , United States )
Batnyam, Uyanga
(
University of Washington
, Seattle , Washington , United States )
Author Disclosures:
Perisa Ashar:DO NOT have relevant financial relationships
| Ketan Tamirisa:DO NOT have relevant financial relationships
| Shriya Garg:No Answer
| Uyanga Batnyam:No Answer