Recent Rise in Ischemic Stroke Mortality with Comorbid Type 2 Diabetes and Associated Demographic Disparities: A Nationwide Study (1999–2020)
Abstract Body (Do not enter title and authors here): Background: Type 2 diabetes (T2D) is a well-established risk factor for ischemic stroke (IS), yet national trends in IS mortality with T2D as a contributing cause remain poorly characterized. Understanding these patterns is essential for informing targeted stroke prevention efforts among high-risk populations.
Research Questions: What are the temporal trends in IS mortality in the United States when T2D is listed as a contributing cause of death? Additionally, how do these mortality trends vary by sex, race, urbanization level, and geographic region?
Methods: We analyzed national mortality data from the CDC WONDER database from 1999 to 2020 for individuals aged >35 years. IS (ICD-10: I63, I69.3) was designated as the underlying cause of death, with T2D (E11.0–E11.9) listed as a contributing cause. Age-adjusted mortality rates (AAMRs) per 1,000,000 population were calculated. Joinpoint regression was used to assess temporal trends and estimate annual percent change (APC).
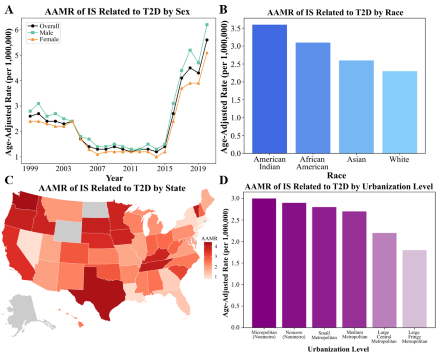
Results: A total of 9,011 IS deaths with comorbid T2D were identified. AAMR declined from 2.6 (95% CI, 2.3–2.8) in 1999 to 1.2 (95% CI, 1.1–1.4) in 2011 (APC = –7.6%; p<0.001), followed by a sharp increase to 5.6 (95% CI, 5.3–6.0) in 2020 (APC = 19.8%; p<0.001). Cumulative AAMR was higher among males (2.7 [95% CI, 2.6–2.7]) than females (2.2 [95% CI, 2.1–2.2]). Racial disparities were evident: American Indians had the highest AAMR (3.6 [95% CI, 2.9–4.5]), followed by African Americans (3.1 [95% CI, 2.9–3.3]), Asians (2.6 [95% CI, 2.3–2.9]), and White individuals (2.3 [95% CI, 2.2–2.4]). Micropolitan rural areas had the highest AAMR (3.0 [95% CI, 2.8–3.2]) compared to large fringe metropolitan areas (1.8 [95% CI, 1.7–1.9]). By region, the West had the highest AAMR (3.2 [95% CI, 3.1–3.3]), followed by the South (2.5 [95% CI, 2.4–2.6]), Midwest (2.5 [95% CI, 2.4–2.6]), and Northeast (1.3 [95% CI, 1.2–1.4]).
Conclusions: After an initial decline, mortality from IS with comorbid T2D has risen markedly since 2011, with disproportionate burden among males, American Indian and African American populations, rural areas, and residents of the Western U.S. These findings highlight the urgent need for integrated strategies focused on diabetes management, stroke prevention, and health equity across high-risk communities.
Ashar, Perisa
(
Duke University
, Durham , North Carolina , United States )
Ajay Jadav, Arnav
(
Washington University in St. Louis
, St. Johns , Florida , United States )
Garg, Shriya
(
University of Georgia
, Athens , Georgia , United States )
Tamirisa, Ketan
(
Washington University in St. Louis
, St. Louis , Missouri , United States )
Batnyam, Uyanga
(
University of Washington
, Seattle , Washington , United States )
Agarwala, Anandita
(
Baylor Scott and White Health
, Plano , Texas , United States )
Author Disclosures:
Perisa Ashar:DO NOT have relevant financial relationships
| Arnav Ajay Jadav:DO NOT have relevant financial relationships
| Shriya Garg:No Answer
| Ketan Tamirisa:DO NOT have relevant financial relationships
| Uyanga Batnyam:DO NOT have relevant financial relationships
| Anandita Agarwala:DO NOT have relevant financial relationships