Effect of Sotatercept on Mortality and Major Morbidity Outcomes in Patients with Pulmonary Arterial Hypertension: Pooled Analysis of the PULSAR, STELLAR, and ZENITH Trials
Abstract Body (Do not enter title and authors here): Introduction: Sotatercept is a first-in-class activin signaling inhibitor that improves the balance between anti- and pro-proliferative signaling in the pulmonary vasculature. Prior double-blind placebo (pbo)-controlled (DBPC) studies have demonstrated the efficacy benefit of sotatercept in participants (pts) with pulmonary arterial hypertension (PAH) in WHO functional class (FC) II–IV, including that sotatercept decreased the risk of mortality and major morbidity outcomes in pts at high risk of death in the recent Phase 3 ZENITH study. The safety profile has been manageable, and monitoring continues in a long-term follow-up study (SOTERIA). Here, we leverage pooled data to further assess mortality and morbidity, including in pts at lower risk of death.
Research Questions/Hypothesis: Analyze mortality and major morbidity outcomes during the complete DBPC periods of 3 sotatercept studies in PAH.
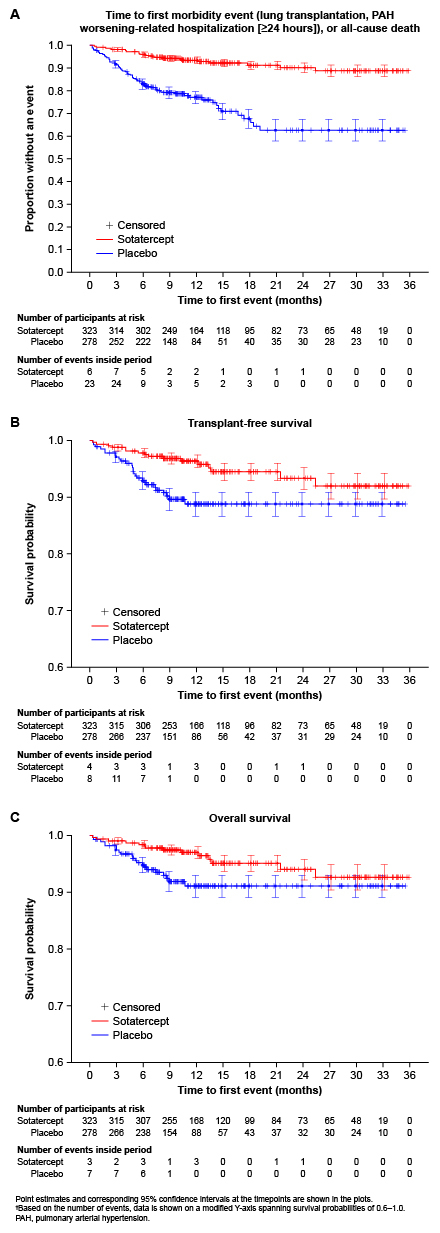
Methods: Data were pooled from pts with PAH receiving background therapy and randomized to sotatercept or pbo in PULSAR (WHO FC II/III; Phase 2; NCT03496207), STELLAR (WHO FC II/III; Phase 3; NCT04576988), and ZENITH (WHO FC III/IV; Phase 3; NCT04896008). This post-hoc analysis comprised (A) time to first morbidity event (lung transplantation, PAH worsening-related hospitalization [≥24 h]), or all-cause death, (B) transplant-free survival (TFS), and (C) overall survival (OS). Hazard ratios (HRs) and 95% confidence intervals (CIs) were generated by Cox proportional hazards models, stratified by study, and P-values by stratified log-rank tests.
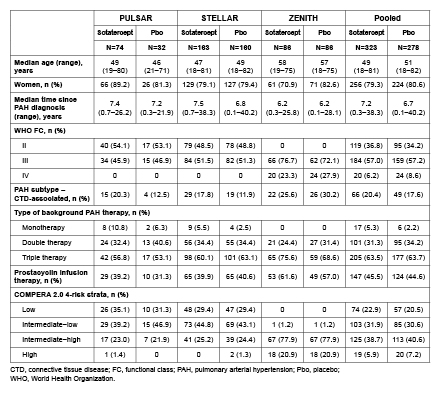
Results: The analysis included 323 pts treated with sotatercept and 278 with pbo. Baseline characteristics were generally comparable between arms, including most having had long-standing PAH (Table 1). Compared with pbo, sotatercept significantly reduced the risk of a first morbidity–mortality event (HR 0.25, 95% CI: 0.16–0.39, P<0.0001; a total of 25 pts had ≥1 event with sotatercept vs 69 pts with pbo), and improved TFS (HR 0.44, 95% CI: 0.24–0.83, P=0.0047; 16 vs 27 pts with ≥1 event) and OS (HR 0.49, 95% CI: 0.25–0.98, P=0.0192; 14 vs 21 pts with ≥1 event) (Fig. 1). By 3–6 months, all 3 Kaplan–Meier curves demonstrated clear separation between treatment arms (Fig. 1).
Conclusions: Sotatercept significantly improved a composite endpoint of mortality and major morbidity outcomes, TFS, and OS, in a pooled analysis of 3 DBPC studies in pts with PAH spanning a broad range of WHO FC, background therapies, and COMPERA risk strata.
Mclaughlin, Vallerie
(
University of Michigan Medical School
, Ann Arbor , Michigan , United States )
Badesch, David
(
University of Colorado
, Aurora , Colorado , United States )