Global Trends in Ischemic Heart Disease Attributable to Kidney Dysfunction: A 204-Country Analysis of Mortality and Disability from 1990 to 2021
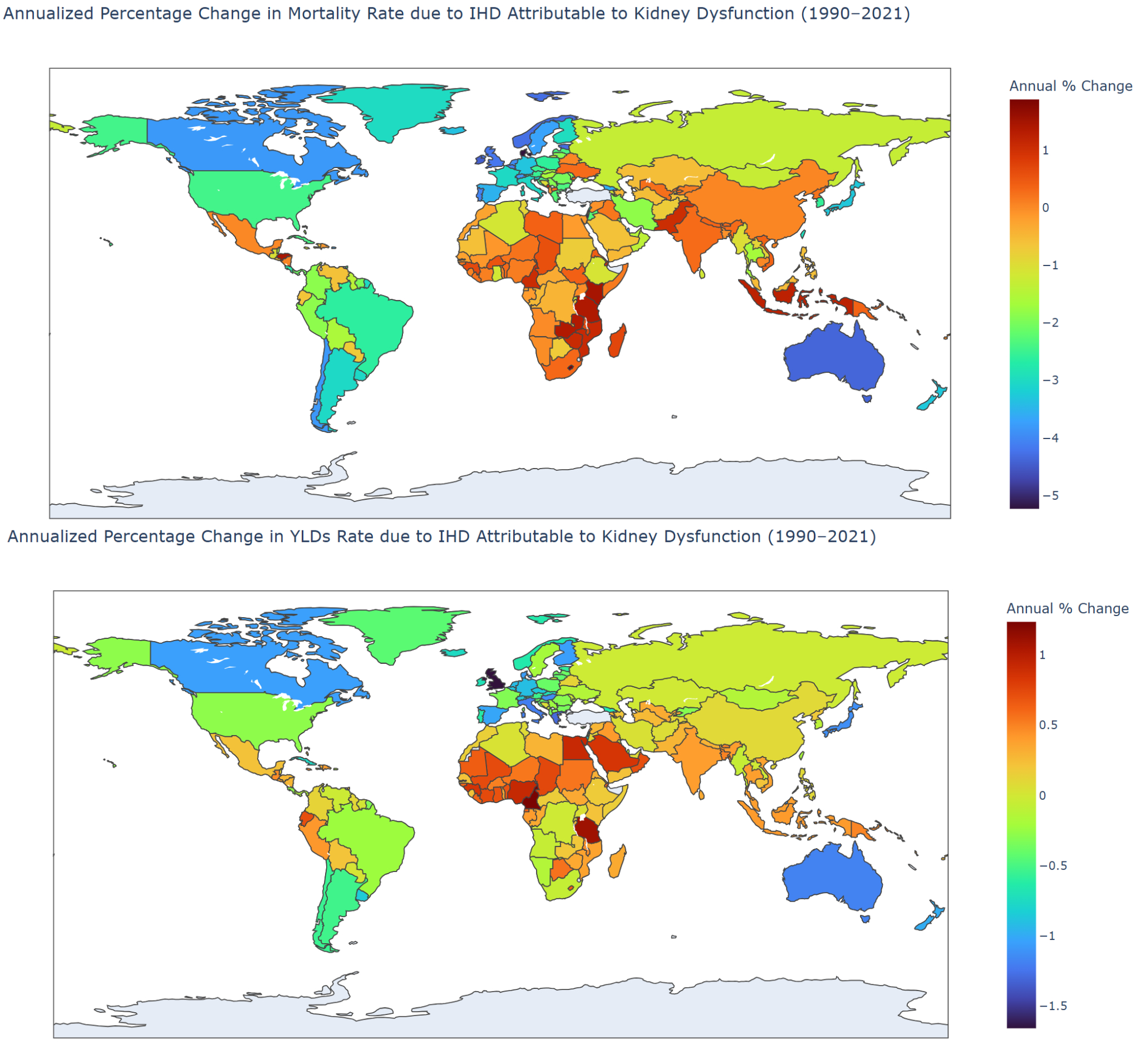
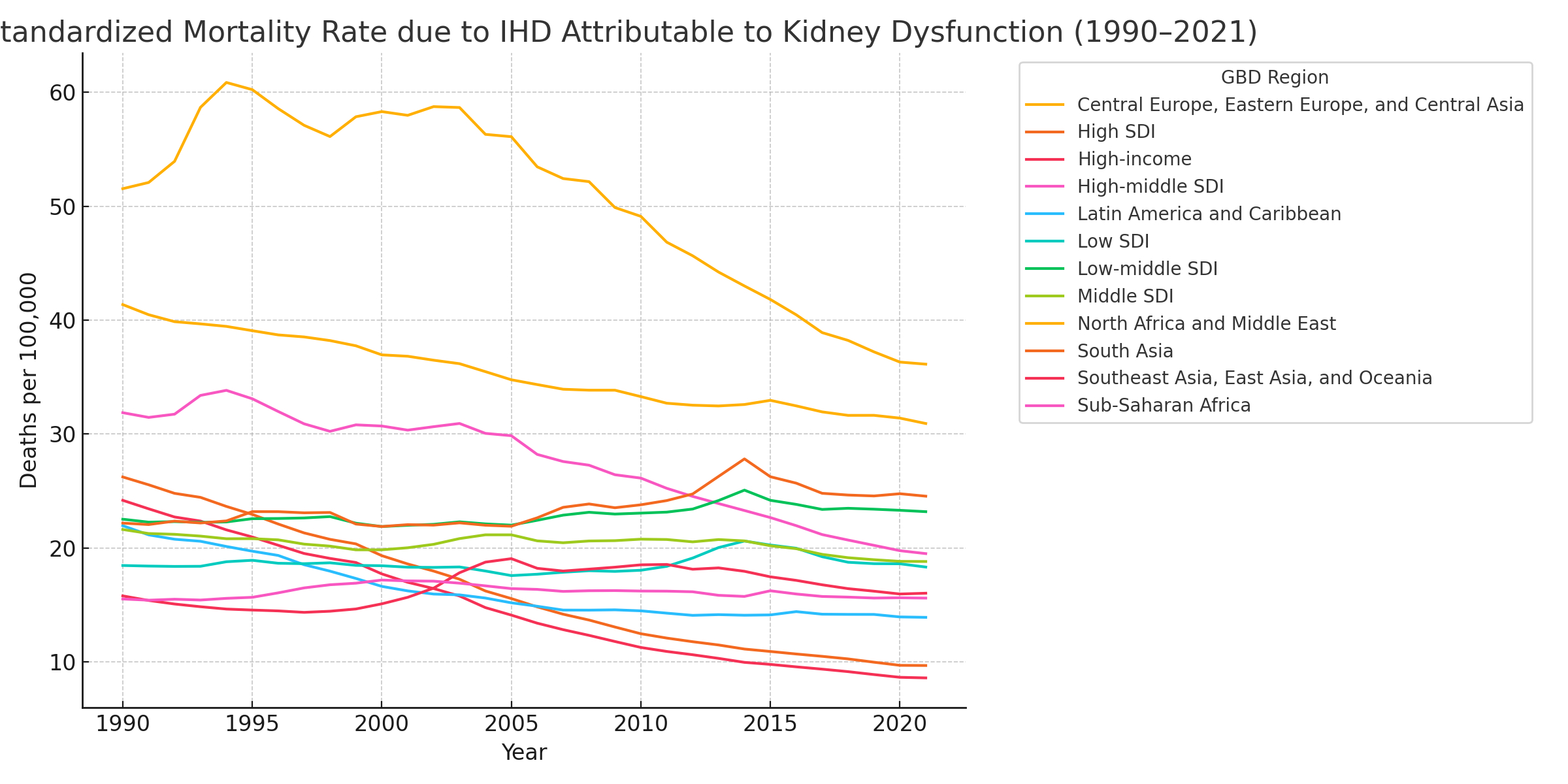
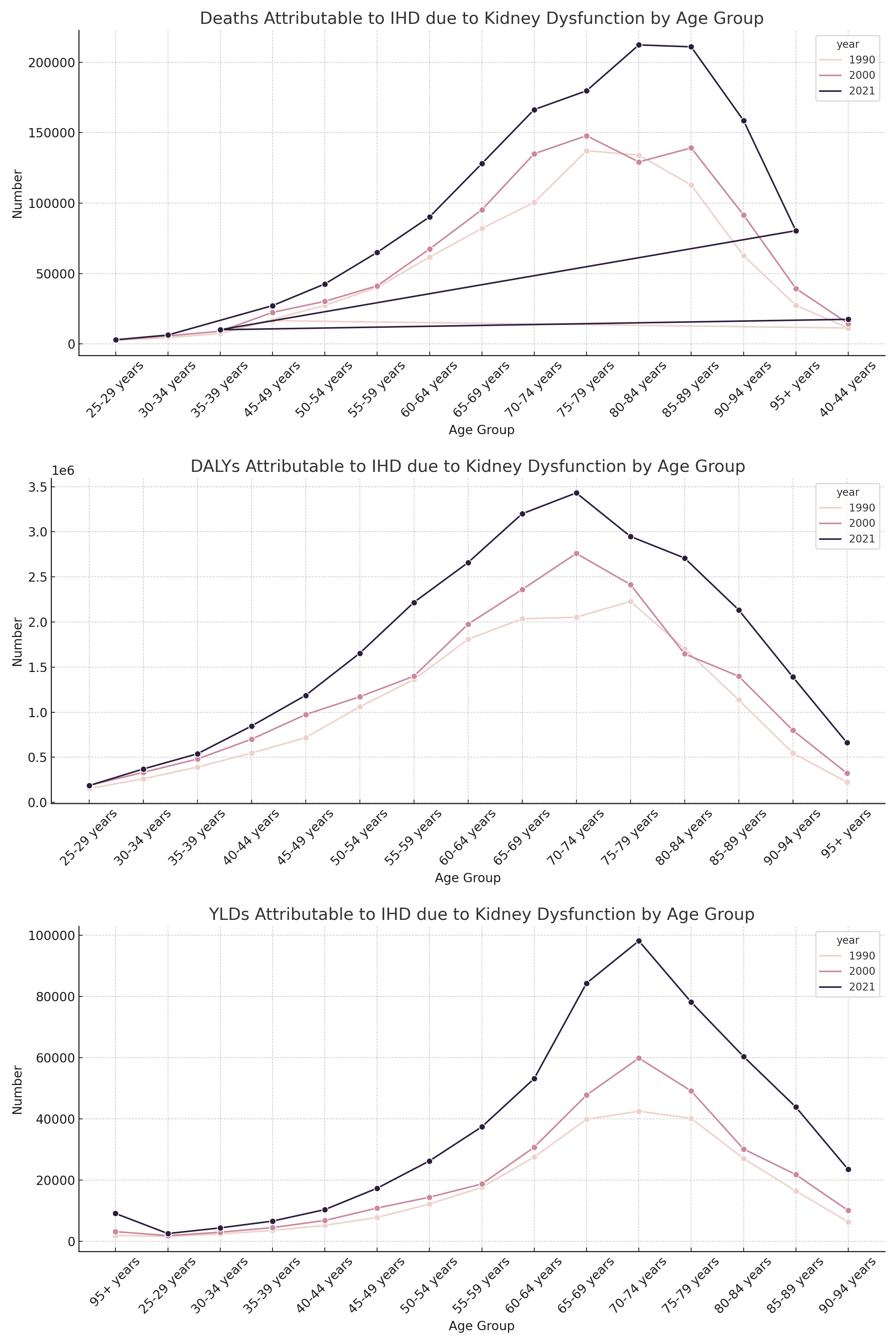
Abstract Body (Do not enter title and authors here): Background: Kidney dysfunction is an under-recognized yet growing contributor to ischemic heart disease (IHD) burden worldwide. As chronic kidney disease (CKD) prevalence rises globally, its cardiovascular sequelae—especially IHD—pose serious challenges to health systems, particularly in low- and middle-income regions. Understanding the long-term burden of IHD attributable to kidney dysfunction is essential for informing global health priorities and integrated disease management strategies. Methods: We analyzed trends in mortality and disability attributable to IHD due to kidney dysfunction across 204 countries and territories from 1990 to 2021 utilizing global burden of disease study 2021 framework. Age-standardized mortality rates (ASMR), Years Lived with Disability (YLDs), and Disability-Adjusted Life Years (DALYs) were extracted. Annualized Percentage Change (APC) was calculated for each measure, and results were stratified by geography, age group, and Socio-Demographic Index (SDI) region. Results: Globally, the APC in ASMR due to IHD attributable to kidney dysfunction ranged from +1.47% in Madagascar to −5.04% in Australia between 1990 and 2021. Sub-Saharan African nations such as Nigeria (+1.24%) and Central African Republic (+1.10%) experienced significant increases, whereas countries like Canada (−3.26%) and Germany (−2.79%) showed notable declines. For YLDs, the APC ranged from +1.18% in Nigeria to −1.56% in Australia, with upward trends clustered in West Africa, South Asia, and parts of Southeast Asia. Age-specific trends revealed a substantial rise in total deaths from 2,420 in the 25–29 age group in 1990 to 14,866 in the 70–74 age group in 2021. DALYs showed similar growth, with 8,890 DALYs in the 40–44 age group in 1990 increasing to 52,189 in the 70–74 age group by 2021. YLDs also increased from 2,756 in the 30–34 age group in 1990 to 9,683 in the 70–74 age group in 2021, indicating an expanding burden of non-fatal disease across aging populations. Conclusion: From 1990 to 2021, mortality and disability due to IHD attributable to kidney dysfunction declined in many high-income countries but increased sharply in Sub-Saharan Africa and parts of Asia. With some countries experiencing APCs exceeding +1% annually, targeted interventions to manage renal risk factors and integrated care models for IHD and CKD are urgently needed, particularly in low-SDI settings facing rising disease burdens.
Nimmalapudi, Dayana Sai Swetha
(
Gandhi Medical College, Secunderabad, Hyderabad, Telangana, India- 500003
, Telangana , India )
Dhanani, Maulik
(
Southwestern University SOM
, Mahwah , Texas , United States )
Gopi, Anaswara
(
Sree Gokulam Medical College and Research Foundation
, Kerala , India )
Viramgama, Fagun
(
Surat Municipal Institute of Medical Education and Research (SMIMER) 395010, India Surat, India
, Surat , India )
Singh, Gurpinderdeep
(
DMCH Ludhiana
, Ludhiana , India )
Patel, Tirth
(
G.M.E.R.S. Medical College
, Ahmedabad , India )
Kotnani, Sandeep
(
Rutgers Monmouth Medical Center
, Monmouth , New Jersey , United States )
Amin, Vishrant
(
JFK University Medical Center
, Milltown , New Jersey , United States )
Desai, Hardik
(
Independent Clinical and Public Health Researcher
, Ahmedabad , GUJARAT , India )
Author Disclosures:
Dayana Sai Swetha Nimmalapudi:DO NOT have relevant financial relationships
| Maulik Dhanani:No Answer
| Anaswara gopi:DO NOT have relevant financial relationships
| Fagun Viramgama:No Answer
| Gurpinderdeep Singh:No Answer
| Tirth Patel:DO NOT have relevant financial relationships
| sandeep kotnani:DO NOT have relevant financial relationships
| VISHRANT AMIN:DO NOT have relevant financial relationships
| HARDIK DESAI:No Answer