Trends and In-Hospital Outcomes of Mechanical Circulatory Support in Heart Failure–Related Cardiogenic Shock: Insights from National Inpatient Sample (2016–2022)
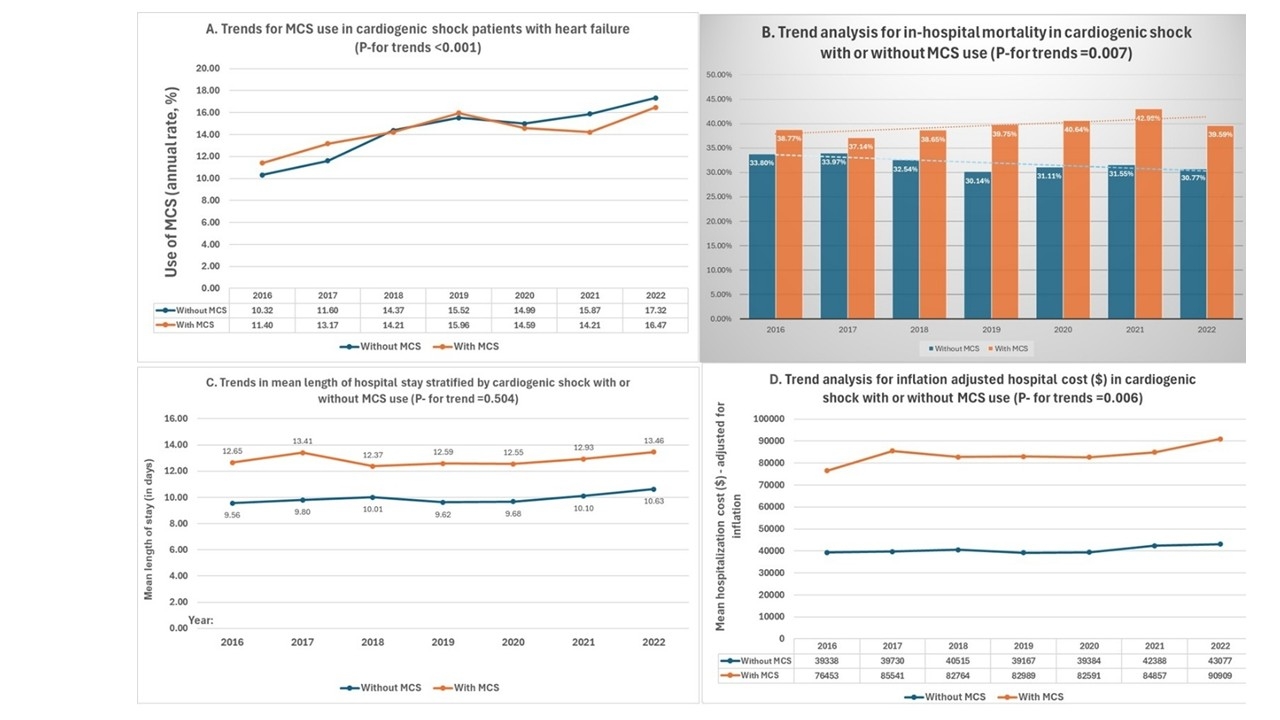
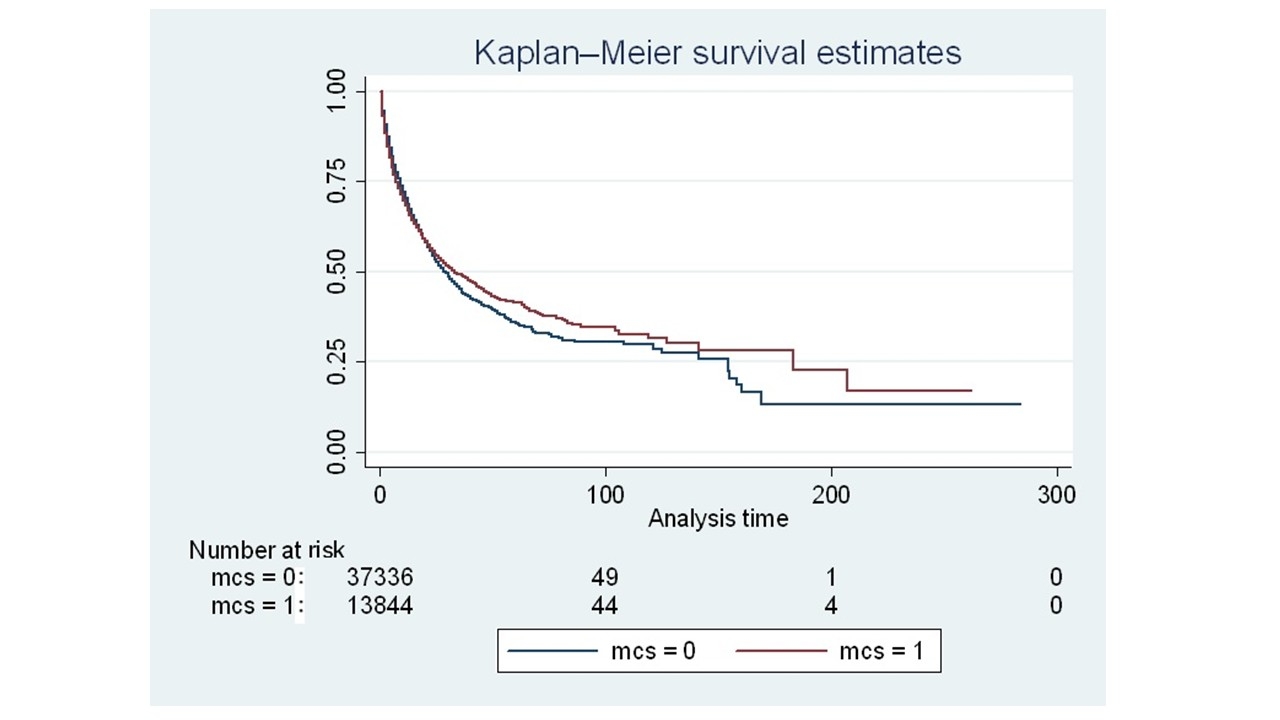
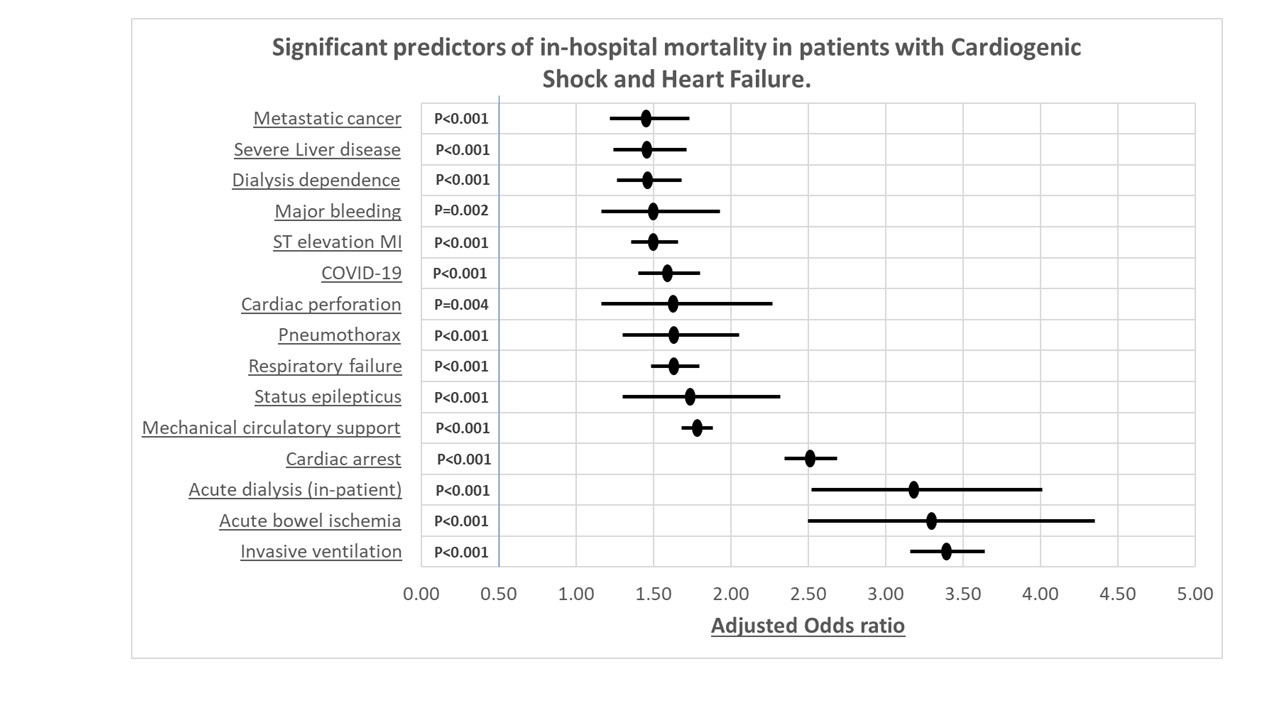
Abstract Body (Do not enter title and authors here): Background: Cardiogenic shock (CS) remains a life-threatening complication in heart failure (HF), often requiring rapid hemodynamic support. Mechanical circulatory support (MCS) devices including intra-aortic balloon pumps (IABP), percutaneous ventricular assist devices (pVADs), and extracorporeal membrane oxygenation (ECMO) have reshaped acute care, yet contemporary national data on utilization trends, outcomes, and disparities in HF-related CS are limited. Objective: To evaluate national trends, outcomes, and disparities in MCS use among patients hospitalized with HF complicated by CS from 2016–2022. Methods: We conducted a retrospective cohort study using the National Inpatient Sample (2016–2022). Adult hospitalizations with a diagnosis of HF and concurrent CS were identified using validated ICD-10-CM codes. MCS use (IABP, Impella, ECMO) was captured and stratified by year. Outcomes included in-hospital mortality, length of stay (LOS), and inflation-adjusted hospitalization costs. Multivariable regression adjusted for demographics, comorbidities, and hospital characteristics. Kaplan-Meier analysis was performed for hospitalizations >30 days. Results: Among 265,910 weighted HF-CS admissions, MCS use increased from 11.4% in 2016 to 16.5% in 2022 (p<0.001). In-hospital mortality remained high but was lower with MCS (31.8%) vs. non-MCS (39.7%). Kaplan-Meier analysis showed improved survival for MCS patients with prolonged hospital stays (log-rank p=0.036). MCS use was associated with longer LOS (13 vs. 10 days, p<0.001) and higher costs ($84,000 vs. $41,000, p<0.001). MCS was more frequently used in younger patients (67.6 vs. 69.7 years, p<0.001) with fewer comorbidities. However, in-hospital deaths were more common in older patients (71 vs. 68 years, p<0.001). Use was higher in urban-teaching hospitals, the Midwest, and among White patients and those in higher income quartiles (p<0.05). Use was lowest in rural and small hospitals. Mechanical ventilation was the strongest mortality predictor in MCS recipients (aOR 2.45; 95% CI, 2.27–2.64). Conclusions: MCS use in HF-related CS has increased nationally, but mortality benefits remain modest, especially in older and ventilated patients. Significant disparities by geography, race, and income persist. These findings underscore the need for equitable access, improved patient selection, and prospective trials to define optimal MCS strategies.
Majid, Muhammad
(
AdventHealth Florida
, Sebring , Florida , United States )
Aamer, Atiya
(
AdventHealth Florida
, Sebring , Florida , United States )
Geffin, Ryan
(
Cleveland Clinic Florida
, Weston , Florida , United States )
Asghar, Muhammad Sohaib
(
AdventHealth
, Sebring , Florida , United States )
Khanna, Radhika
(
Cleveland Clinic Florida
, Weston , Florida , United States )
Agrawal, Ankit
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Reddi, Vuha
(
Cleveland Clinic Florida
, Weston , Florida , United States )
Shimshak, Thomas
(
AdventHealth Florida
, Sebring , Florida , United States )
Klein, Allan
(
CLEVELAND CLINIC
, Cleveland , Ohio , United States )
Author Disclosures:
Muhammad Majid:DO NOT have relevant financial relationships
| Atiya Aamer:No Answer
| Ryan Geffin:DO NOT have relevant financial relationships
| Muhammad Sohaib Asghar:DO NOT have relevant financial relationships
| Radhika Khanna:No Answer
| Ankit Agrawal:No Answer
| Vuha Reddi:DO NOT have relevant financial relationships
| Thomas Shimshak:No Answer
| Allan Klein:DO NOT have relevant financial relationships