Combined left- and right-sided native valve infective endocarditis with no predisposing risk factors or intracardiac shunt
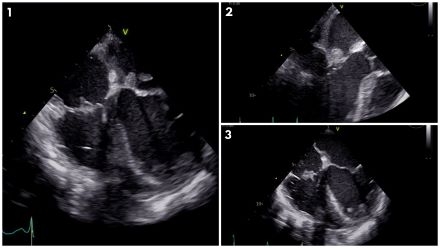
Abstract Body (Do not enter title and authors here): Combined left and right-sided Infective Endocarditis (IE) is rare and typically occurs with underlying predisposing factors such as intravenous drug use, presence of hemodialysis catheters, congenital defects, and intracardiac devices. We present a 62-year-old woman with diabetes, hypertension, and severe peripheral vascular disease, diagnosed with combined left- and right-sided native valve IE despite lack of typical underlying risk factors. She presented with altered mental status and sepsis; blood cultures were positive for Streptococcus group G. Initial transthoracic echocardiogram revealed an 8 mm echogenicity on the atrial aspect of the mitral valve. Subsequently, a transesophageal echocardiogram was performed, revealing a large (2 x 0.9 cm) highly mobile mass on the anterior leaflet of the mitral valve with mild to moderate mitral regurgitation (Figures 1,2); additionally, a small size (0.9 x 0.7 cm) highly mobile mass was seen on the tricuspid valve with mild tricuspid regurgitation (Figures 1,3), meeting criteria for combined left- and right-sided infective endocarditis. The patient was assessed by the cardiothoracic team, and due to presence of multiple comorbidities the risk of surgery was deemed to outweigh the benefits for valve replacement or repair. Therefore, she was treated medically with broad-spectrum antibiotics with subsequent significant improvement and did not develop any complications throughout her hospital stay. IE has an incidence of 3–10 cases per 100,000 annually in developed countries, with Staphylococcus aureus as the most common pathogen. Tricuspid valve IE accounts for 5–10% of cases. Although rare, combined left and right-sided IE can develop without underlying risk factors as in our clinical case. Multivalvular IE also poses greater risk for severe complications, including valvular dysfunction, heart failure, abscess formation, and conduction abnormalities, as well as systemic and pulmonary embolization, contributing to high morbidity. This case illustrates the importance of early diagnosis and individualized treatment in rare presentations of combined IE. It highlights that conservative, non-surgical management can be effective in select patients and supports the need for further research to guide treatment strategies in complex IE cases.
Inshyna, Diana
(
Brookdale Hospital Medical Center
, Brooklyn , New York , United States )
Almakadma, Abdul Hakim
(
Brookdale University Hospital
, Brooklyn , New York , United States )
Saeidifard, Farzane
(
Brookdale Hospital Medical Center
, Brooklyn , New York , United States )
Author Disclosures:
Diana Inshyna:DO NOT have relevant financial relationships
| Abdul Hakim Almakadma:DO NOT have relevant financial relationships
| Farzane Saeidifard:No Answer