Association of Catheterization Timing with In-Hospital Outcomes in OHCA Patients with NSTEMI: A National Analysis
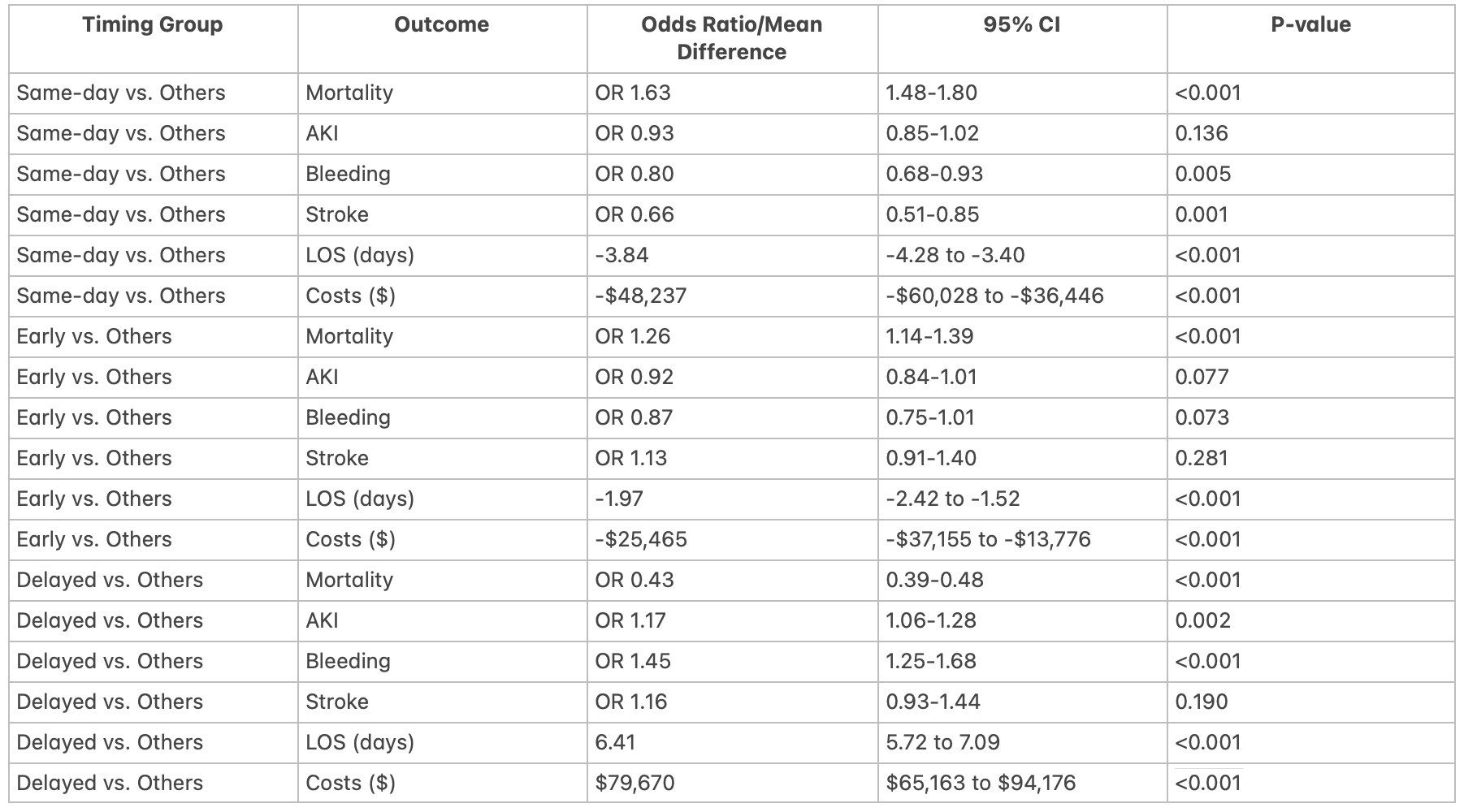
Abstract Body (Do not enter title and authors here): Background: The optimal timing of cardiac catheterization in patients experiencing out-of-hospital cardiac arrest (OHCA) presenting with non-ST-elevation myocardial infarction (NSTEMI) remains controversial. This study aimed to evaluate associations between catheterization timing and clinical outcomes in a large, contemporary national cohort. Methods: Using the National Inpatient Sample (2016–2022), we studied 9,068 adult OHCA patients with NSTEMI undergoing cardiac catheterization (~45,000 hospitalizations nationwide). Patients were grouped by catheterization timing: same-day, early (1–2 days), or delayed (≥3 days). Outcomes included in-hospital mortality, AKI, bleeding, stroke, LOS, and costs. Entropy balancing and survey-weighted regression adjusted for confounders. Results: Same-day catheterization was associated with higher in-hospital mortality (odds ratio [OR] 1.63; 95% confidence interval [CI], 1.48–1.80; p<0.001), but lower risks of bleeding (OR 0.80; 95% CI, 0.68–0.93; p=0.005), stroke (OR 0.66; 95% CI, 0.51–0.85; p=0.001), shorter LOS (-3.84 days; 95% CI, -4.28 to -3.40; p<0.001), and reduced costs (-$48,237; 95% CI, -$60,028 to -$36,446; p<0.001). Early catheterization (1–2 days) similarly showed increased mortality (OR 1.26; 95% CI, 1.14–1.39; p<0.001). Delayed catheterization (≥3 days) correlated with lower mortality (OR 0.43; 95% CI, 0.39–0.48; p<0.001) but increased risks of AKI (OR 1.17; 95% CI, 1.06–1.28; p=0.002), bleeding (OR 1.45; 95% CI, 1.25–1.68; p<0.001), longer LOS (+6.41 days; 95% CI, 5.72–7.09; p<0.001), and higher hospitalization costs (+$79,670; 95% CI, $65,163–$94,176; p<0.001). Conclusion: In this observational national cohort study, early cardiac catheterization (within 2 days) was associated with increased in-hospital mortality despite advantages in complication rates, LOS, and costs. Delayed catheterization correlated with reduced mortality but higher morbidity and resource utilization. Further prospective research is required to identify patient-specific criteria and optimal intervention timing, considering neurological status and other unmeasured factors like contrast volumes etc. due to inherant limitations of NIS influencing outcomes.
Ahluwalia, Vibhor
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Jaiswal, Jay
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Bhatia, Smriti
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Dutta, Abhishek
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Murillo-garcia, David
(
Towerhealth
, Reading , Pennsylvania , United States )
Singer, Robert
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Dhar, Sunil
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Author Disclosures:
Vibhor Ahluwalia:DO NOT have relevant financial relationships
| Jay Jaiswal:DO NOT have relevant financial relationships
| Smriti Bhatia:No Answer
| Abhishek Dutta:DO NOT have relevant financial relationships
| David Murillo-Garcia:No Answer
| Robert Singer:DO NOT have relevant financial relationships
| Sunil Dhar:No Answer