The Statin Shortfall: Lower Statin Use in Autoimmune Disease Despite Elevated Cardiovascular Risk Across LDL-C Levels.
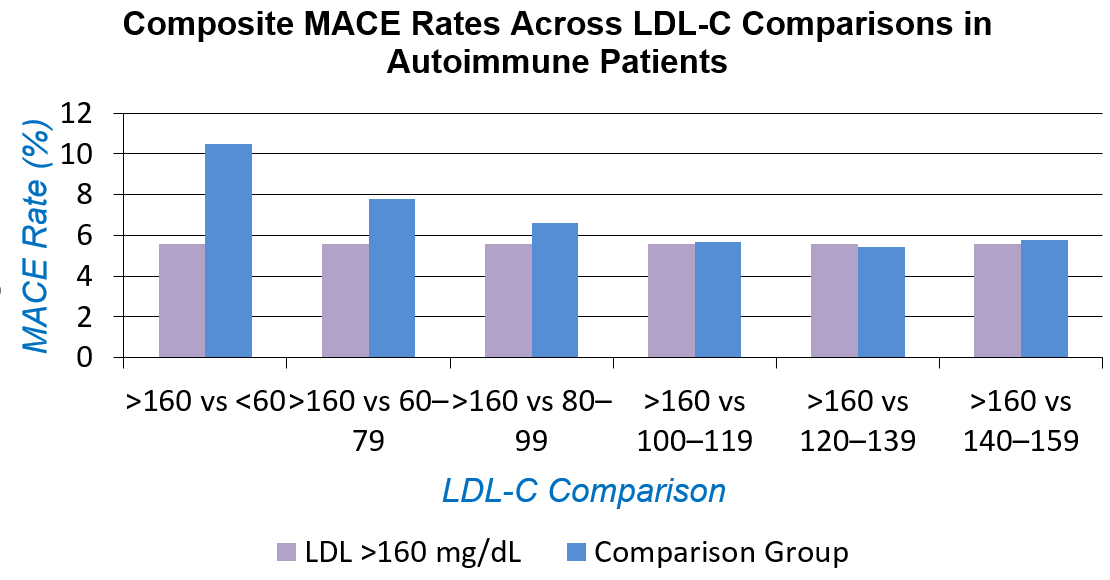
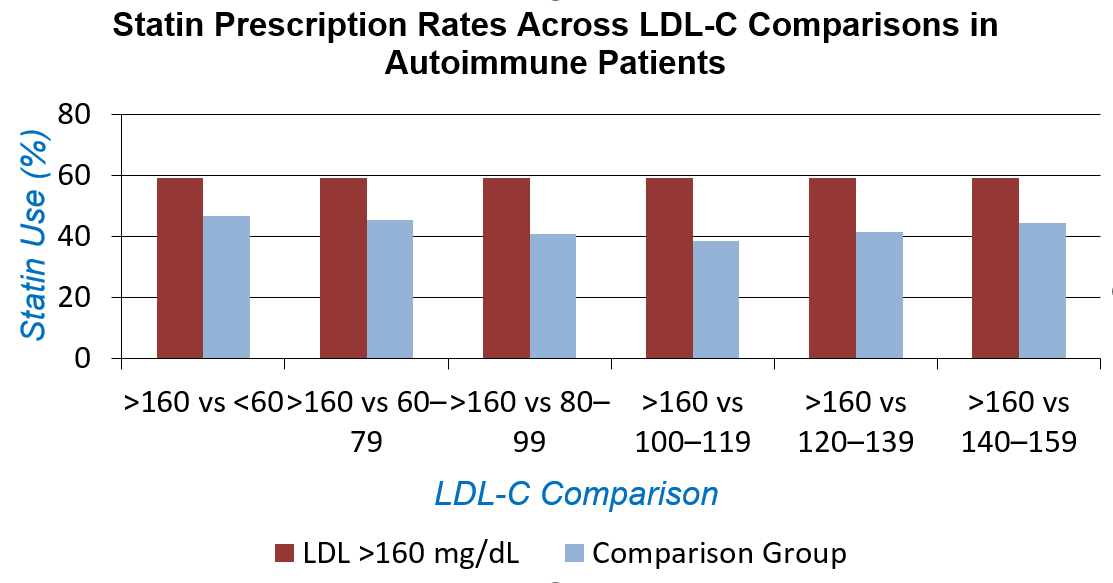
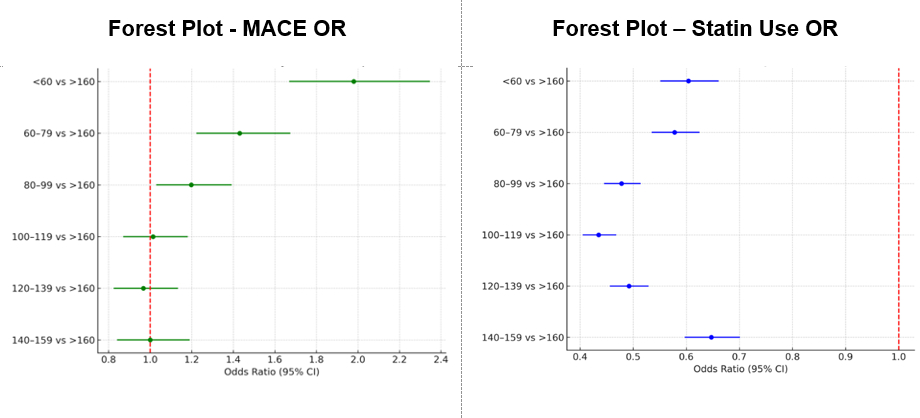
Abstract Body (Do not enter title and authors here): Background: It is well known that patients with autoimmune conditions such as rheumatoid arthritis and systemic lupus erythematosus are at increased risk for atherosclerotic cardiovascular disease. However, contemporary patterns of lipid-lowering therapy in autoimmune disease, especially among those with low LDL-C, remain inadequately defined. Hypothesis: We hypothesized that statin therapy is underutilized in autoimmune patients with lower LDL-C levels despite similar or elevated risk of major adverse cardiovascular events (MACE). Methods: Using the TriNetX platform, which provides real-time, deidentified clinical data from the electronic medical records, we conducted a nationwide retrospective cohort analysis of adult patients (≥18 years) with rheumatoid arthritis or systemic lupus erythematosus, stratified by LDL-C into seven groups: <60, 60–79, 80–99, 100–119, 120–139, 140–159, and ≥160 mg/dL. The MACE outcomes defined as myocardial infarction, stroke, coronary revascularization, or cardiovascular death and the respective statin usage were compared between each group and the ≥160 mg/dL reference group using odds ratios (ORs) with 95% confidence intervals. Results: A total of 50,436 autoimmune patients were included. Among patients with autoimmune disease, statin use was consistently lower across all lower LDL-C strata when compared to those with LDL-C >160 mg/dL. The odds ratios (OR) for statin use ranged from 0.435 (95% CI: 0.405–0.468) in the 100–119 mg/dL group to 0.647 (95% CI: 0.597–0.701) in the 140–159 mg/dL group, indicating a substantial treatment gap. In contrast, the risk of major adverse cardiovascular events (MACE) was significantly higher among autoimmune patients with lower LDL-C levels relative to those with LDL-C >160 mg/dL. The highest odds were observed in the <60 mg/dL group (OR 1.980, 95% CI: 1.669–2.347), followed by the 60–79 mg/dL (OR 1.431, 95% CI: 1.222–1.675) and 80–99 mg/dL (OR 1.198, 95% CI: 1.029–1.393) groups. No statistically significant differences in MACE risk were observed in the higher LDL-C strata.
Conclusion: Among autoimmune patients, statin therapy is markedly underprescribed in those with lower LDL-C levels, despite persistent or elevated cardiovascular risk. These findings suggest that current LDL-C–based thresholds may inadequately capture cardiovascular risk in autoimmune populations and support the need for broader risk-based treatment strategies.
Jaganathan, Vijayadithyan
(
University of Nevada Reno School Of Medicine
, Reno , Nevada , United States )
Mendpara, Vaidehi
(
Cleveland Clinic Foundation
, Cleveland , Ohio , United States )
Maturi, Bhanu
(
University of Texas Health Science Center at Houston
, Houston , Texas , United States )
Venugopalan, Sruthi
(
University of Nevada Reno School Of Medicine
, Reno , Nevada , United States )
Ramesh, Prasana
(
UMass Chan - Baystate
, Springfield , Massachusetts , United States )
Wassif, Heba
(
Cleveland Clinic Foundation
, Cleveland , Ohio , United States )
Author Disclosures:
Vijayadithyan Jaganathan:DO NOT have relevant financial relationships
| Vaidehi Mendpara:DO NOT have relevant financial relationships
| Bhanu Maturi:DO NOT have relevant financial relationships
| Sruthi Venugopalan:DO NOT have relevant financial relationships
| Prasana Ramesh:DO NOT have relevant financial relationships
| heba wassif:DO NOT have relevant financial relationships