Dual-Chamber Leadless Pacemaker Implantation in an Orthotopic Heart and Kidney Transplant Recipient With ESRD and Transient Atrial Non-Capture
Abstract Body (Do not enter title and authors here): Background Leadless pacemakers offer advantages in immunosuppressed patients or those with limited venous access. This case highlights the novel use of a dual-chamber leadless pacemaker (DC-LP) in a patient with a complex history: orthotopic heart transplant (OHT), kidney transplant (KT), and now end-stage renal disease (ESRD) on intermittent hemodialysis (iHD) via a left arm arteriovenous fistula (AVF). The procedure was complicated by transient atrial non-capture after atrial lead deployment.
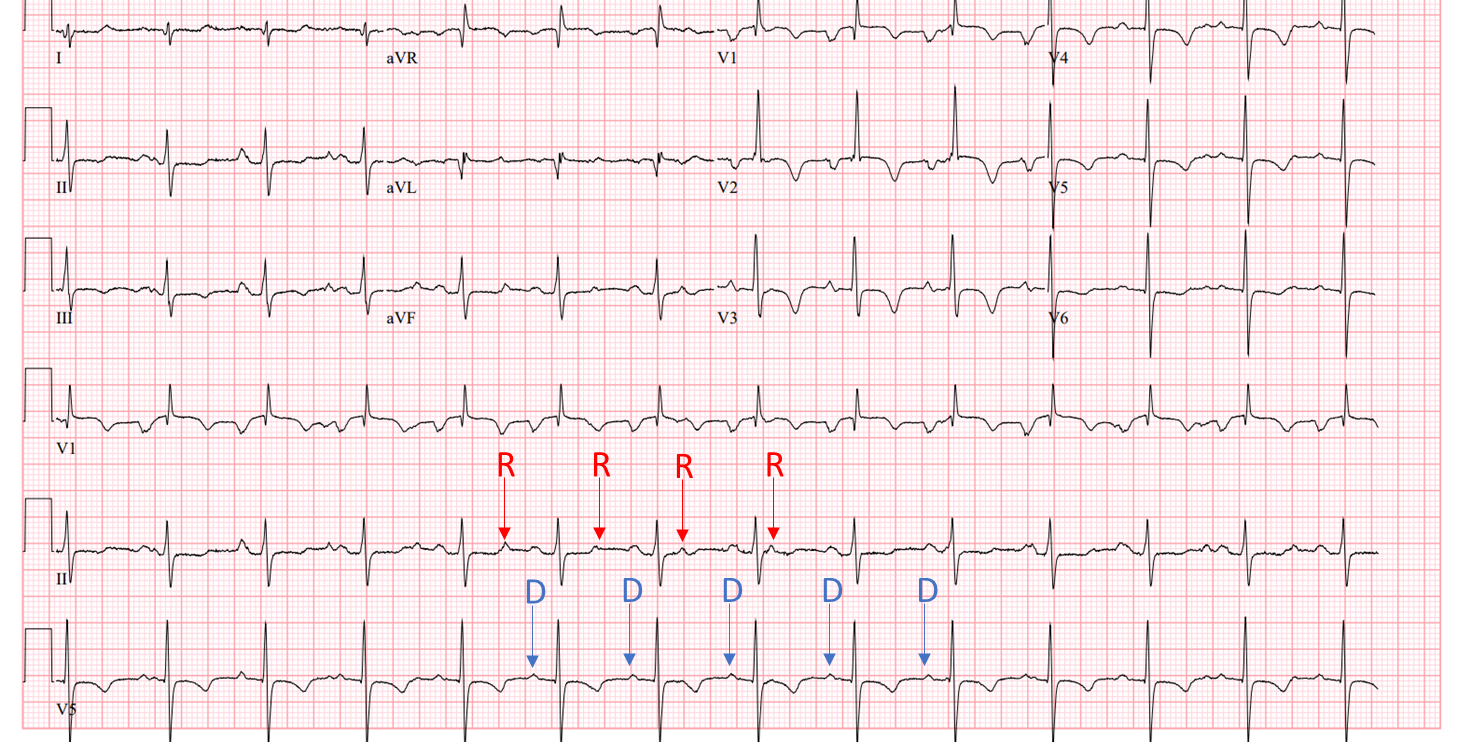
Description of Case A 31-year-old male with a history of parvovirus myocarditis status-post OHT and prior KT—complicated by multiple graft rejections, now on iHD for ESRD via a left arm AVF, presented with bradycardia and hypotension during iHD. He denied chest pain or syncope but endorsed exertional fatigue. ECG revealed complete heart block with a junctional escape rhythm and AV dissociation. Two distinct P-wave morphologies suggested dual atrial activity from residual native tissue and donor sinus node.
Echocardiogram showed normal LV systolic function (EF 60–65%), mild to moderate RV dilation with mildly reduced function, and elevated RV systolic pressure. Coronary angiography showed no allograft vasculopathy, biopsy revealed mild (1R) rejection. Dopamine transiently improved sinus rate and AV conduction.
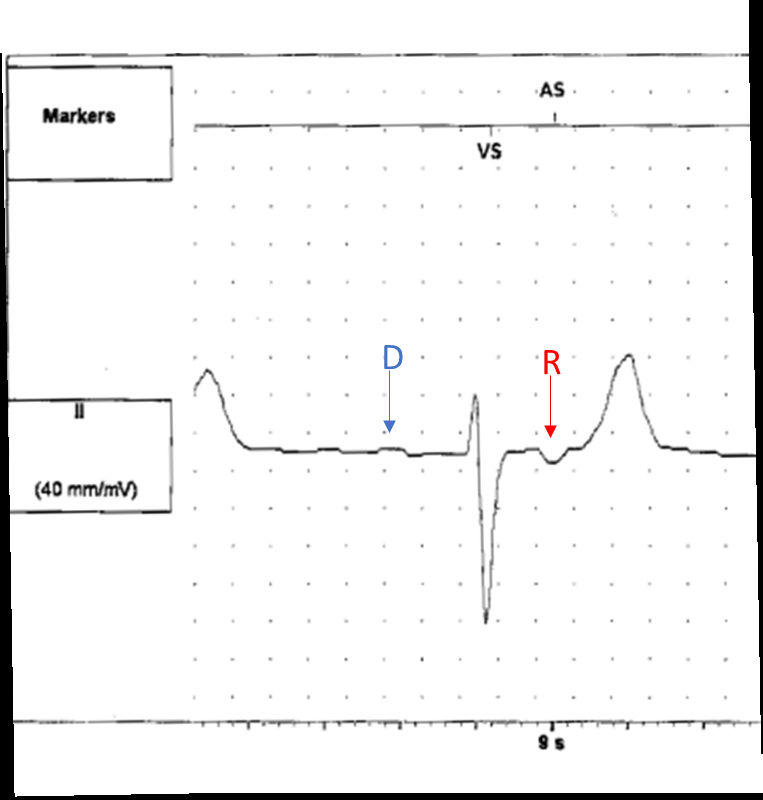
Due to persistent chronotropic incompetence, a DC-LP was implanted. The decision was driven by his KT history, current iHD, and left arm AVF – factors rendering venous preservation and infection risk reduction critical. Following atrial lead deployment, transient atrial non-capture was noted but resolved spontaneously, likely due to local tissue effects at the implant site. Final programming was AAI70/VVI40.
Discussion This is, to our knowledge, the first reported DC-LP case in a patient with both OHT and KT. His complex profile—including immunosuppression, failed renal graft, left arm AVF, and ESRD—made him ideal for leadless pacing. DC-LP minimizes infection risk, preserves venous access, and avoids lead-related complications. The transient atrial non-capture likely related to local tissue injury, resolved spontaneously, underscoring the modality’s reliability in complex cases.
Conclusion DC-LP is a feasible and beneficial option for transplant recipients. This case demonstrates the successful DC-LP use in a patient with OHT, KT, iHD dependence, and left arm AVF, while emphasizing the importance of recognizing post-implant pacing anomalies that may self-resolve.
Vilarino, Valerie
(
University of Miami
, Miami , Florida , United States )
D'ovidio, Tyler
(
University of Miami
, Miami , Florida , United States )
Rubin, Phillip
(
University of Miami
, Miami , Florida , United States )
Mohan, Chaitra
(
Jackson Memorial Hospital
, Miami , Florida , United States )
Author Disclosures:
Valerie Vilarino:DO NOT have relevant financial relationships
| Tyler D'Ovidio:DO NOT have relevant financial relationships
| Phillip Rubin:DO NOT have relevant financial relationships
| Chaitra Mohan:No Answer