Abstract Body (Do not enter title and authors here):
Background: In coronary hemodynamics, laminar flow is a protective mechanism, and turbulent flow is a detrimental factor. In clinical practice, for patients with unstable angina, the necessity of intervention for moderate lesions (50-70% stenosis) is always questioned. In this study, we comprehensively evaluated the risk factors that may lead these plaques to progress to myocardial infarction using angiography, IVUS, and Deep Learning.
Hypothesis: Vulnerable lesions are usually associated with plaque eccentricity and stagnant flow, causing chest pain.
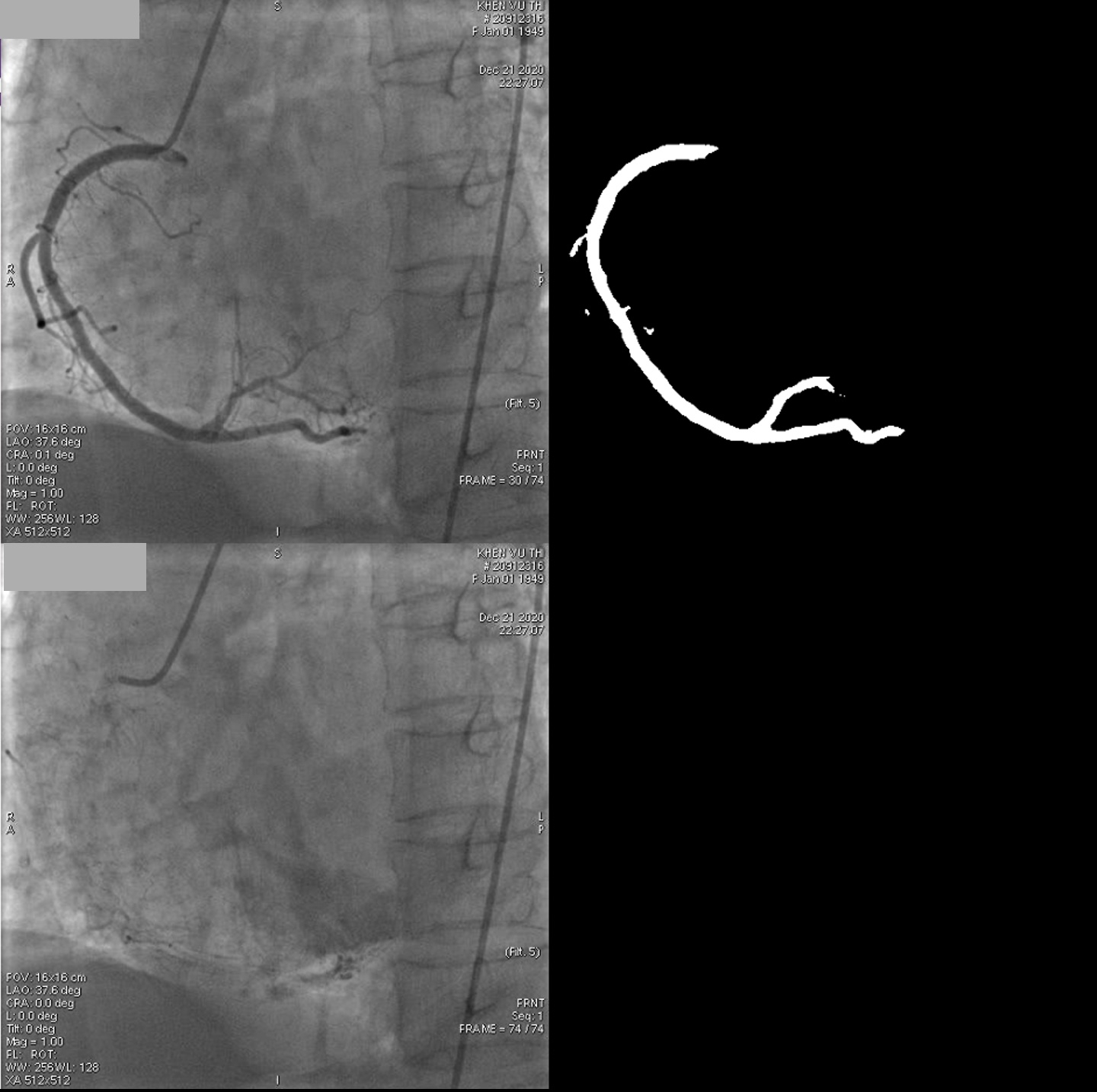
Methods: Patients with a single lesion admitted with diagnosed of unstable angina underwent the dynamic angiographic technique with IVUS support. First, the coronary artery was fully injected with contrast. After the injection stopped, the blood (white) began streaming in to replace the contrast (black). The flow characteristics and movements will be recorded through the disappearance of the contrast opacity with 15 frames/second. In aditionally, the arterial phase (AP) was calculated as the time from frames with full contrast to frames with washed-out contrast. Moreover, IVUS was performed for evaluate plaque features (eccentricity, calcification and vulnerable). At the same time, deep learning (DL) models were built based on independent datasets (225 angiogram videos). The DL program was constructed using a combination of U-Net and DenseNet-121. The segmentation model and a convolutional neural network were used to detect the starting frame, ending frame of AP.
Results: Fifty patients met inclusion criteria (72% males) with a mean age of 66.2 ± 9.5 years. IVUS analysis revealed that 84% (42 patients) had plaque eccentricity without (or minimal) calcification. Contrast stagnation was observed for a longer duration in eccentric coronary regions compared to non-eccentric plaque regions, as quantified by DL analysis of the arterial phase (24.5 +/- 1.6 frames vs 30.1+/- 1.4 frames, p < 0.05). After stenting, the stagnant flow was eliminated, and flow was restored to 25 ± 2.1 frames.
Conclusion: Plaque eccentricity along with a prolonged arterial phase (stagnant flow) are causes of chest pain in unstable angina. This is a personalized indication for PCI, even if they are moderate lesions.