Polycythemia Vera as an Underrecognized Cause of Aortic Dissection in a Patient Without Traditional Cardiovascular Risk Factors
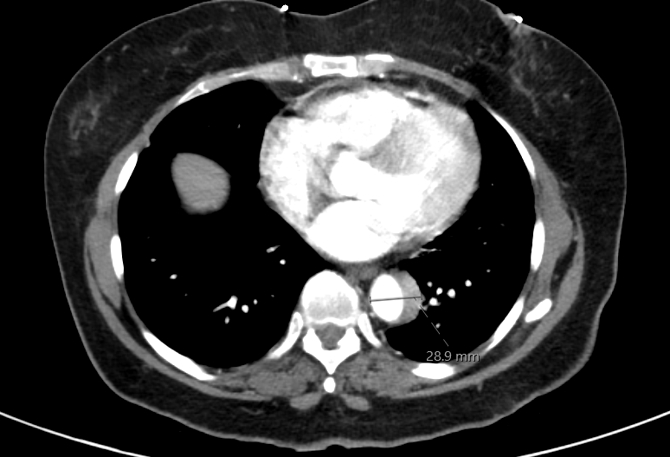
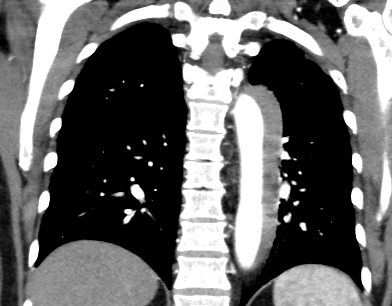
Abstract Body (Do not enter title and authors here): Aortic dissection is a life-threatening condition most commonly associated with chronic hypertension, connective tissue disorders, and atherosclerosis. Polycythemia vera (PV), a chronic myeloproliferative neoplasm, is an uncommon but important secondary cause of vascular pathology due to its prothrombotic state, endothelial dysfunction, and associated hypertension. We present a case of acute Stanford type B aortic dissection in a previously healthy patient, ultimately diagnosed with PV. A 70-year-old woman with no cardiovascular history presented with sudden-onset, severe substernal chest pain radiating to the back while doing yard work, associated with diaphoresis, shortness of breath, and right-hand paresthesia. She was a never-smoker and denied alcohol or drug use. At urgent care, her blood pressure was 196/174 mmHg. After receiving aspirin and sublingual nitroglycerin, she was transferred to the ED with persistent back pain (BP 186/110 mmHg). D-dimer was 1.49. ECG showed no ischemia. CTA revealed a Stanford type B aortic dissection extending from the distal arch to the aortic hiatus. She was started on IV esmolol and nicardipine and transferred for vascular surgery evaluation. TTE showed normal LV ejection fraction (65–70%), grade 1 diastolic dysfunction, and moderate concentric LV hypertrophy. She was managed conservatively without surgery, transitioned to oral antihypertensives, and scheduled for surveillance follow-up to monitor for progression. Initial labs showed elevated hemoglobin (18.2 g/dL) and hematocrit (58.9%), prompting outpatient evaluation. Hematologic workup revealed low erythropoietin (1.8 mIU/mL) and a positive JAK2 V617F mutation, confirming polycythemia vera. She was started on hydroxyurea, low-dose aspirin, and serial phlebotomy. Hematocrit and BP normalized, and repeat CTA at 3 months showed complete resolution of the dissection. This case illustrates polycythemia vera as a rare but significant contributor to aortic dissection. In PV, hyperviscosity, increased shear stress, and endothelial dysfunction can lead to vascular complications even in the absence of traditional risk factors. The patient’s hypertensive emergency and dissection were likely precipitated by undiagnosed PV. This underscores the importance of considering myeloproliferative disorders in patients presenting with unexplained erythrocytosis and vascular pathology. Early diagnosis and cytoreductive therapy may reduce the risk of life-threatening cardiovascular events.
Vellanki, Sravya
(
Willis Knighton Health
, Shreveport , Louisiana , United States )
Muppidi, Harshini
(
Willis Knighton Health
, Shreveport , Louisiana , United States )
Virani, Ahmed
(
Willis Knighton Health
, Shreveport , Louisiana , United States )
Author Disclosures:
Sravya Vellanki:DO NOT have relevant financial relationships
| Harshini Muppidi:No Answer
| Ahmed Virani:DO NOT have relevant financial relationships