Race Differences in Acute Chest Pain Care in a Multisite U.S. Cohort
Abstract Body (Do not enter title and authors here): Introduction: Race-based differences in cardiovascular care are well described. However, data examining differences in cardiac testing and death or myocardial infarction (MI) rates among U.S. emergency department (ED) patients with acute chest pain by race are limited.
Research Question: Do safety and healthcare utilization differ by race among patients with chest pain in a multisite U.S. ED cohort?
Methods: We conducted a multisite observational study using the Wake Forest Chest Pain Registry, including patients ≥18 years old who were evaluated for possible acute coronary syndrome from 1/1/2021–12/31/2021 across 25 EDs. Each ED used the same high-sensitivity troponin protocol for chest pain evaluations. Race was determined by patient self-report in the electronic health record and reported as White non-Hispanic, Black non-Hispanic, Hispanic, and Other. The primary safety outcome was 30-day all-cause death or MI. Healthcare utilization outcomes included 30-day hospitalizations and objective cardiac testing (OCT), which was defined as non-invasive testing (NIT: stress testing and coronary computed tomography angiography) and invasive coronary angiography. Outcomes between races were compared using chi-square tests. Multivariable logistic regression models were used to assess the association between race and outcomes adjusting for sex, age, obesity, smoking, rurality, prior coronary artery disease, diabetes, hypertension, hyperlipidemia, insurance status, ED site, and initial troponin, with White race as the reference group.
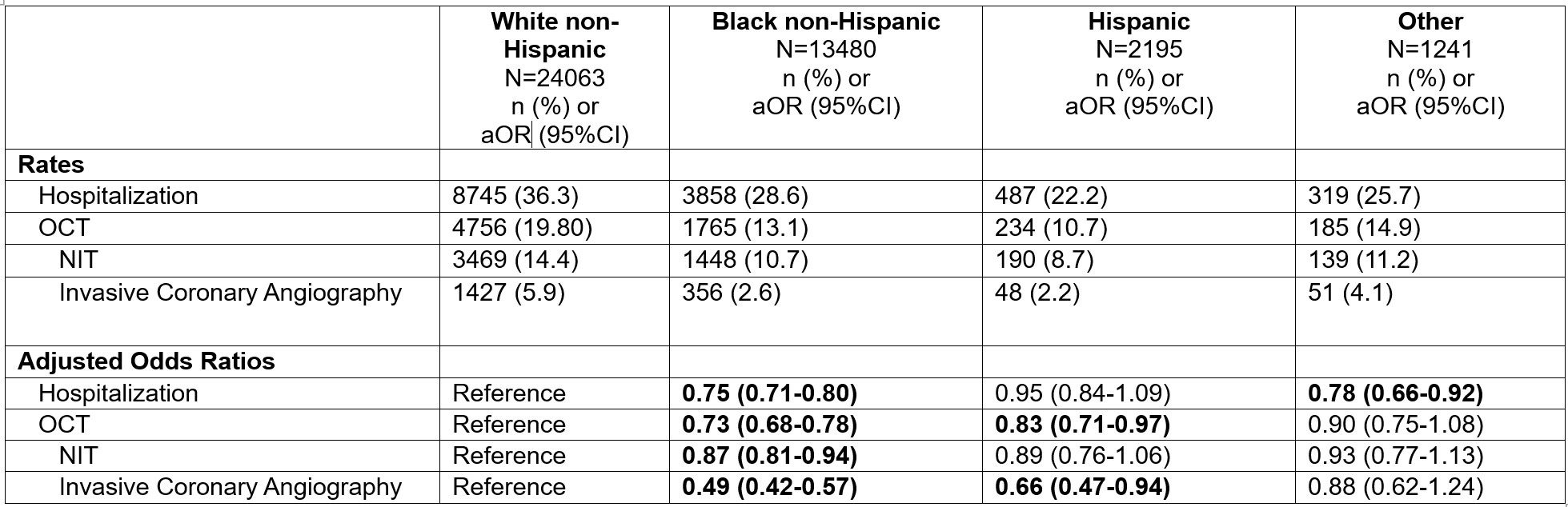
Results: Among 40979 patients, 58.7% were White, 32.9% Black, 5.4% Hispanic, and 3.0% Other. At 30 days, death or MI occurred in 4.6% (1,097/24063) of White patients compared to 2.2% (301/13480) of Black and 1.6% (36/2195) of Hispanic patients (p<0.001). Compared to White patients, the odds of 30-day death or MI were lower among Black (aOR 0.51, 95%CI: 0.43-0.60) and Hispanic (aOR 0.65, 95%CI: 0.44-0.97) patients. OCT at 30 days occurred in 19.8% (4756/24063) of White, 13.1% (1765/13480) of Black, and 10.7% (234/2195) of Hispanic patients (p<0.001). Compared to White patients, after adjusting for confounders, the odds of 30-day OCT were lower among Black (aOR 0.73, 95%CI: 0.68-0.78) and Hispanic (aOR 0.83, 95%CI: 0.71-0.97) patients. Table 1 describes OCT and hospitalization rates by race.
Conclusion: Black and Hispanic patients with chest pain had lower rates of 30-day death or MI and OCT compared to White patients.
Jean-louis, Richard
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Snavely, Anna
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Ashburn, Nicklaus
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Paukner, Lyle
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Supples, Michael
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Hutchison, Benjamin
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Mcknight, Kyle
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Higgins, Max
(
Wake Forest School of Medicine
, Winston-Salem , North Carolina , United States )
Pearson, David
(
Atrium Health Carolina's Medical Center
, Charlotte , North Carolina , United States )
Mahler, Simon
(
WAKE FOREST SCHOOL MEDICINE
, Winston Salem , North Carolina , United States )
Author Disclosures:
Richard Jean-Louis:DO NOT have relevant financial relationships
| Simon Mahler:DO have relevant financial relationships
;
Advisor:Abbott :Active (exists now)
; Consultant:QuidelOrtho:Past (completed)
; Ownership Interest:Impathiq:Active (exists now)
; Researcher:Beckman Coulter:Past (completed)
; Researcher:Siemens:Past (completed)
; Research Funding (PI or named investigator):Roche:Active (exists now)
; Research Funding (PI or named investigator):Abbott:Active (exists now)
; Advisor:Siemens:Past (completed)
; Advisor:Polymedco:Active (exists now)
| Anna Snavely:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Abbott Laboratories:Active (exists now)
| Nicklaus Ashburn:DO NOT have relevant financial relationships
| Lyle Paukner:No Answer
| Michael Supples:No Answer
| Benjamin Hutchison:No Answer
| Kyle McKnight:DO NOT have relevant financial relationships
| Max Higgins:No Answer
| David Pearson:DO have relevant financial relationships
;
Advisor:Powerful Medical Inc:Active (exists now)
; Ownership Interest:Powerful Medical Inc:Active (exists now)