Pulmonary congestion assessment by automated quantitative computer tomography in heart failure patients
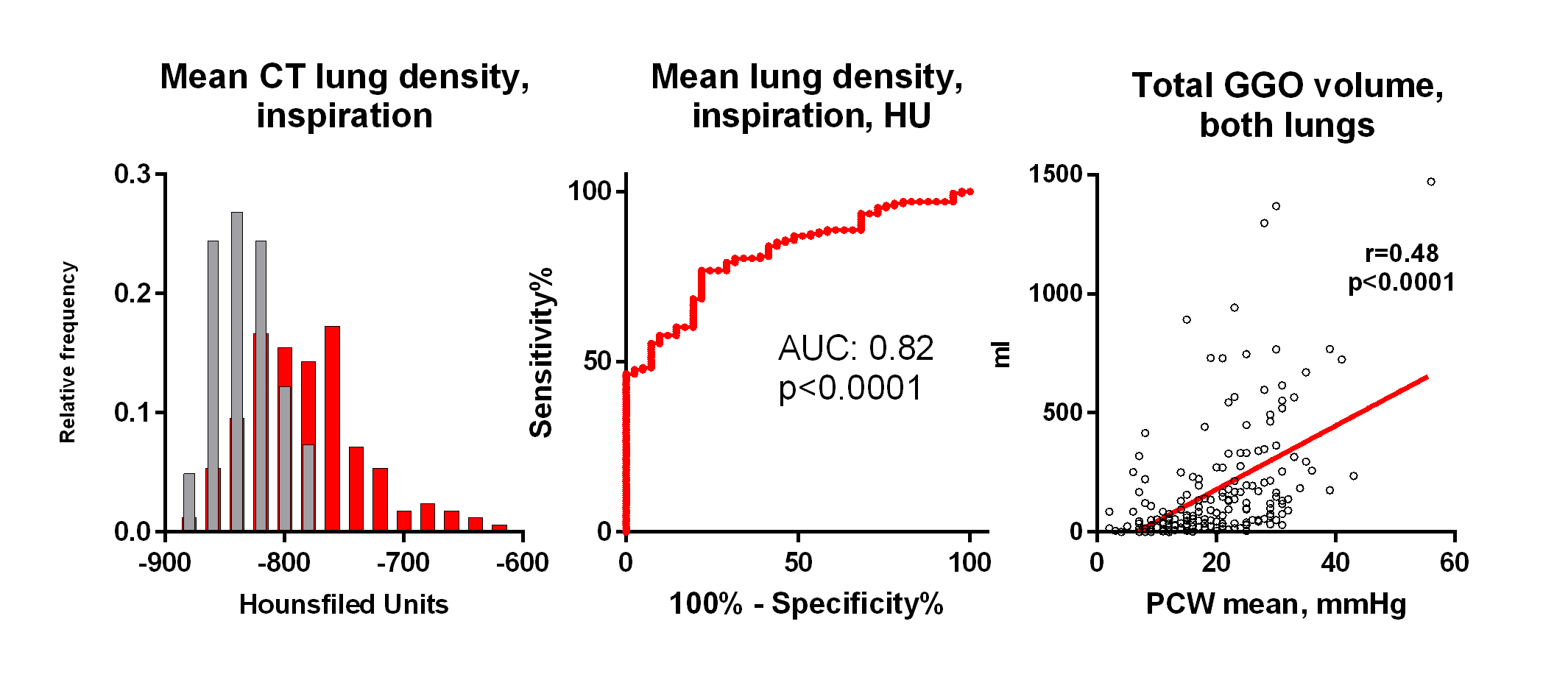
Abstract Body (Do not enter title and authors here): Introduction: Heart failure (HF) affects interstitial lung structure and function. AI-assisted quantitative computed tomography (qCT) offers possibility of objective assesment of lung structure, allowing to detect the presence and the severity of HF. Hypothesis: Can automated qCT analysis discriminate HF from controls and identify tissue structures most linked to degree of congestion ? Methods: Subjects underwent right heart catheterization (RHC), native CT chest imaging (full inspiration/expiration) by Naeotom-α photon-counting CT scanner (Siemens), lab testing, echocardiography. Automated AI-based analysis (VIDA Diagnostics) was employed to evaluate lung volumes, densities and tissue texture. Image series were used in mediastinal and lung window reconstruction with slice thickness 0,8 mm and increments 0,5 mm. Results: 186 HF patients (85% HFrEF, NYHA 2.8±0.5, 58 y, 80% males, NTproBNP 4491 pg/ml, LVEF 26%) and 43 controls of similar sex and BMI were analyzed; both groups free of primary lung disease. In HF, 85 % had PH (mPAP>20mmHg). HF patients had comparable inspiratory lung volume, reduced air volume and increased lung tissue volume, compared to controls. Mean lung density (-782±50 vs -832±25 HU, p<0.0001), density variability and estimated lung fluid content (21.3 vs 16.7%, p<0.0001) were all higher in HF compared to controls. Across various density cut-offs, the most notable difference was at lung tissue density < -856 HU at inspiration. Lung tissue density corelated with mean PA pressure (r=0.49, p<0.0001), and less with pulmonary vascular resistance (r=0.21, p=0.006). Insp/exp scan analysis showed no difference in air trapping, but reduced lung tissue compliance (Jacobian strain: 1.8±0.4 vs 1.6±0.3, p=0.0005) in HF. Lung texture analysis showed increased ground-glass opacity (GGO) mass (48.8 g vs 9.1 g; p < 0.001), reticulation (42.2 g vs. 8.4 g; p < 0.001) and consolidation (0.5 g vs 0.2 g; p=0.0011) in HF compared to controls, with no difference in honeycombing. GGO mass correlated strongly with pulmonary capillary wedge pressure (PCWP) (r=0.48, p<0.001) and mitral regurgitation grade (r=0.28,<0.0001), but not with inflammation (hsCRP, IL6, WBC), smoking exposure or oncotic pressure. Conclusions: qCT distinguished HF patients from controls by increased lung tissue mass, reduced air volume, increased lung density and increased mass of GGO and reticulation. GGO mass in HF strongly reflects increased hydrostatic pressure, but not inflammation.
Melenovsky, Vojtech
(
Institute for Clinical and Experimental Medicine - IKEM
, Prague , Czechia )
Jenca, Dominik
(
Institute for Clinical and Experimental Medicine - IKEM
, Prague , Czechia )
Adla, Theodor
(
Institute for Clinical and Experimental Medicine - IKEM
, Prague , Czechia )
Yarnykh, Svetlana
(
Institute for Clinical and Experimental Medicine - IKEM
, Prague , Czechia )
Al Hiti, Hikmet
(
Institute for Clinical and Experimental Medicine - IKEM
, Prague , Czechia )
Binova, Jana
(
Institute for Clinical and Experimental Medicine - IKEM
, Prague , Czechia )
Peterson, Sam
(
VIDA diagnostics
, Coralville , Iowa , United States )
Newell, John
(
VIDA diagnostics
, Coralville , Iowa , United States )
Hoffman, Eric
(
UNIV OF IOWA COLLEGE OF MED
, Iowa City , Iowa , United States )
Borlaug, Barry
(
MAYO CLINIC
, Rochester , Minnesota , United States )
Author Disclosures:
Vojtech Melenovsky:DO have relevant financial relationships
;
Consultant:Novo Nordisk:Active (exists now)
; Research Funding (PI or named investigator):Regeneron:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Consultant:Merck:Active (exists now)
| Barry Borlaug:DO have relevant financial relationships
;
Research Funding (PI or named investigator):NIH/NHLBI:Active (exists now)
; Consultant:Tin Alley Ventures:Active (exists now)
; Consultant:VADovations:Active (exists now)
; Consultant:ShouTi:Active (exists now)
; Consultant:NGMBio:Active (exists now)
; Consultant:Novo Nordisk:Active (exists now)
; Consultant:Merck:Active (exists now)
; Consultant:Janssen:Active (exists now)
; Consultant:Eli Lilly:Active (exists now)
; Consultant:Edwards Lifesciences:Active (exists now)
; Consultant:Boehringer Ingelheim:Active (exists now)
; Consultant:Aria:Active (exists now)
; Consultant:Amgen:Active (exists now)
; Research Funding (PI or named investigator):Tenax Therapeutics:Active (exists now)
; Research Funding (PI or named investigator):Rivus Pharmaceuticals:Active (exists now)
; Research Funding (PI or named investigator):Novo Nordisk:Active (exists now)
; Research Funding (PI or named investigator):Medtronic:Active (exists now)
; Research Funding (PI or named investigator):Corvia:Active (exists now)
; Research Funding (PI or named investigator):AstraZeneca:Active (exists now)
; Research Funding (PI or named investigator):Axon:Active (exists now)
; Research Funding (PI or named investigator):DoD:Active (exists now)
| Dominik Jenca:No Answer
| Theodor Adla:DO NOT have relevant financial relationships
| Svetlana Yarnykh:No Answer
| Hikmet Al Hiti:No Answer
| Jana Binova:No Answer
| Sam Peterson:No Answer
| John Newell:DO have relevant financial relationships
;
Consultant:VIDA Diagnostics Inc:Active (exists now)
; Royalties/Patent Beneficiary:Elsevier Publishing Co:Active (exists now)
; Royalties/Patent Beneficiary:VIDA Diagnostics:Active (exists now)
; Individual Stocks/Stock Options:VIDA Diagnostics:Active (exists now)
; Advisor:VIDA Diagnostics Inc:Active (exists now)
| Eric Hoffman:No Answer