Excess of anything is detrimental - unraveling role of multiple accessory renal arteries in Pickering syndrome.
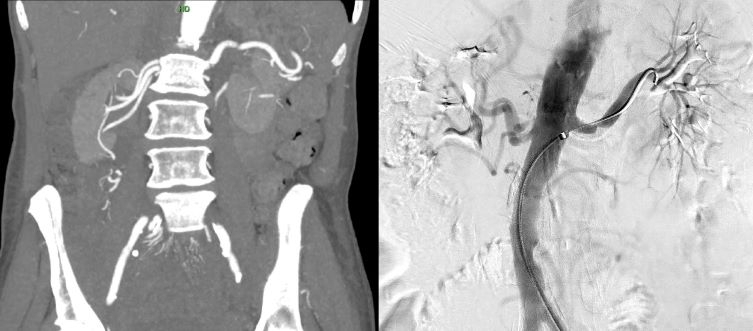
Abstract Body: Flash pulmonary edema (FPE) appears to be more common in patients with bilateral renal artery stenosis (RAS) as compared to those with unilateral disease. The combination of bilateral RAS and recurrent FEP has been named the Pickering syndrome. Here, we present a case of Pickering syndrome caused by unilateral RAS in combination with multiple accessory renal arteries (ARA). To our knowledge, this case marks the inaugural report within the literature. A 68-year-old woman presented to ER with her third episode of FPE in two months, accompanied by hypertensive emergency, BP 232/127 mmHg. Initial evaluation, including laboratory tests and RA ultrasound, showed no abnormalities. However, a CTA of the abdomen revealed a single heavily calcified L main RA with severe atherosclerosis extending into the lumen of the aorta and the proximal L main RA. Three RAs supply R kidney with questionable stenosis of superior, smaller R RA. Atherosclerotic plaque is present at the origin of the inferior R RA, but no definitive significant stenosis is detected. Unilateral RAS and multiple ARAs were suspected to cause HTN and FPE. An aortogram with possible RA stenting was recommended by vascular surgery. It confirmed > 75% stenosis in the L RA, prompting stent deployment. However, no significant stenosis was observed in R ARAs. Post-procedure BP control was achieved with a single agent. FPE is a life-threatening syndrome. Cardiac systolic or diastolic dysfunctions usually accompany it. Recurrent FPE due to bilateral RAS was described by Pickering et al. in 1988. Although its exact mechanism is not completely understood, it is believed to result from excessive fluid volume due to decreased sodium excretion. A similar mechanism was proposed in RAS in a single functional kidney. Could the presence of an ARA mimic the pathophysiology of RAS? It has been theorized that an ARA may lead to HTN due to reduced blood flow to the kidney, caused by its longer and narrower caliber, which increases resistance and may lead to stenosis. The Poiseuille equation, rearranged to R=8μL/ΔPπR4 (where R=resistance, μ=viscosity, L=vessel's length, P=pressure, R=vessel's radius), suggests that both the radius and the length of ARAs may play a role in our patient's condition. In summary, ARAs are a common anatomical variation, and depending on their specific characteristics, they may contribute to resistant HTN and FPE through renin-dependent hyperaldosteronism.
Harris, Liliia
(
Hamilton Medical Center
, Dalton , Georgia , United States )
Zahid, Zaid
(
Hamilton Medical Center
, Dalton , Georgia , United States )
Bains, Nimrat
(
Hamilton Medical Center
, Dalton , Georgia , United States )
Author Disclosures:
Liliia Harris:DO NOT have relevant financial relationships
| Zaid Zahid:DO NOT have relevant financial relationships
| Nimrat Bains:No Answer