QRS duration, aerobic exercise treatment, and risk of hospitalization and mortality in patients with heart failure with reduced ejection fraction; a secondary analysis of the HF-ACTION trial.
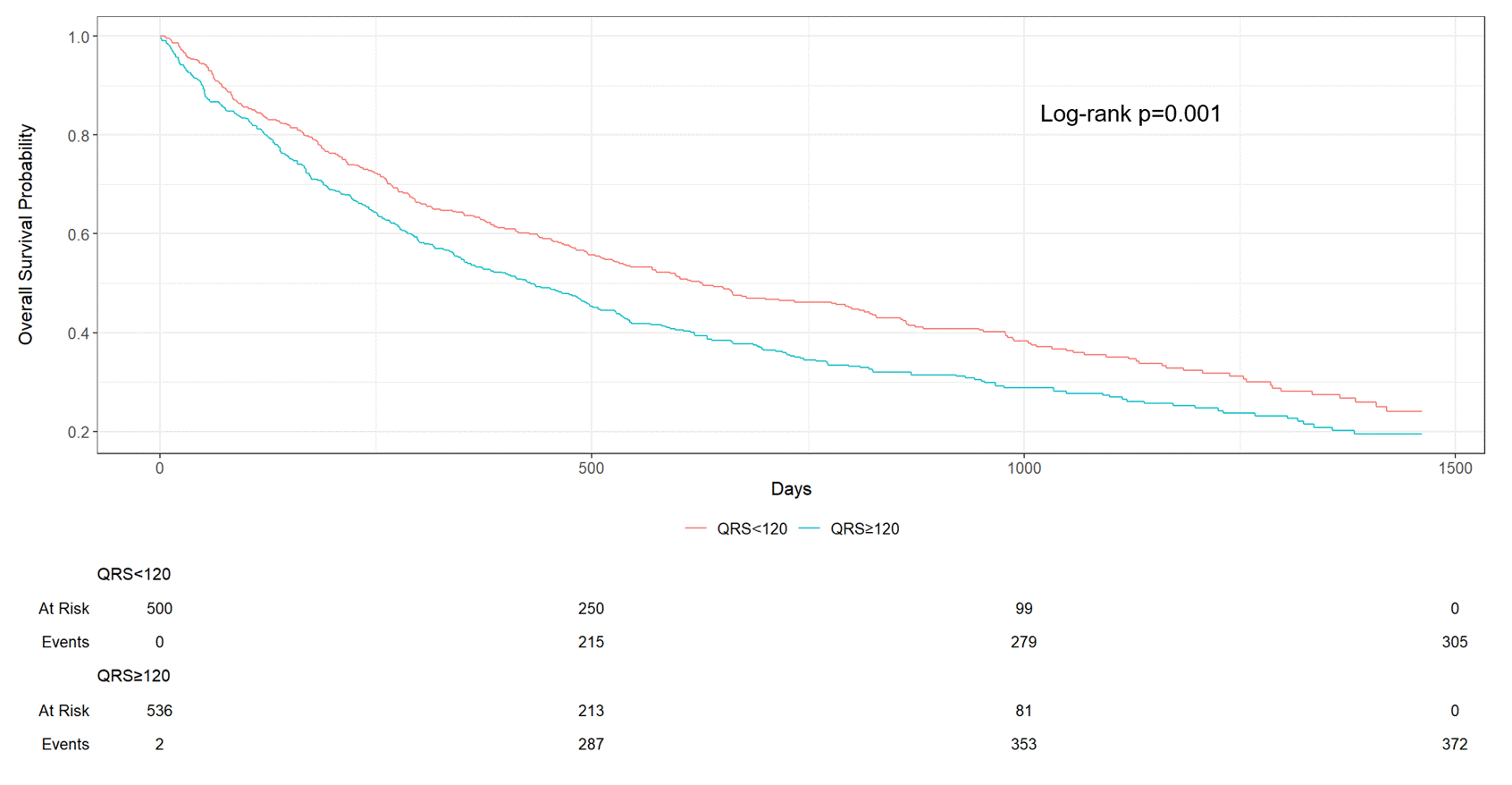
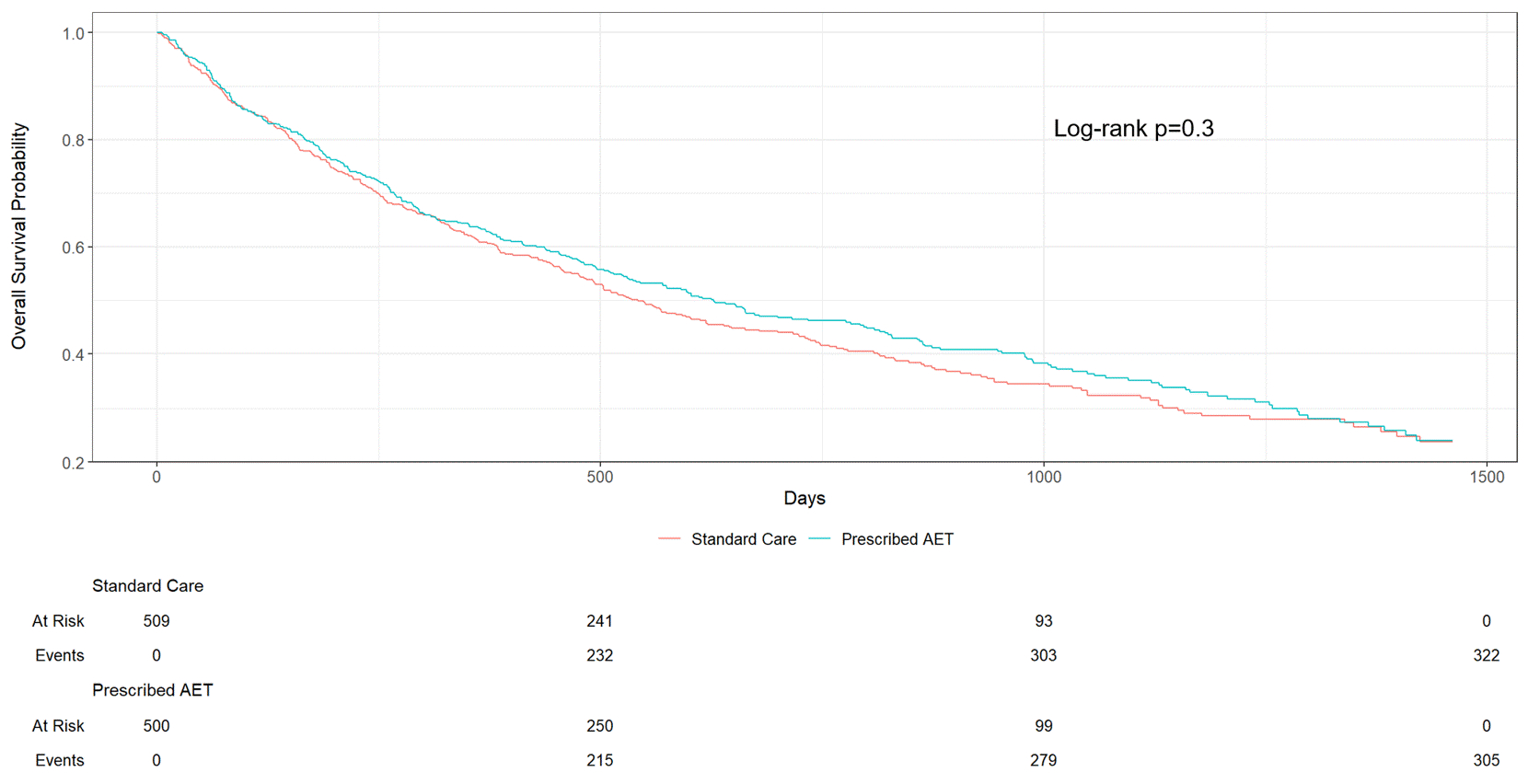
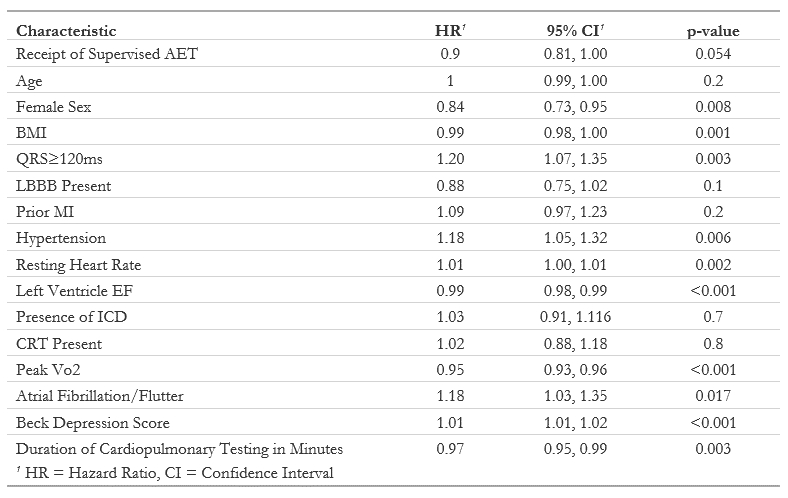
Abstract Body (Do not enter title and authors here): Background: Aerobic exercise training (AET) improves quality of life in patients with heart failure with reduced ejection fraction (HFrEF). Conversely, QRS prolongation increases risk of morbidity and mortality in HFrEF patients. The effect of baseline QRS duration on morbidity and mortality in patients with HFrEF receiving AET has not been explored. Hypothesis: HFrEF patients receiving AET with prolonged QRS are at higher risk for adverse events when compared to controls with normal QRS. Goals/Aims: We aimed to assess differences in survival among patients with HFrEF receiving AET with QRS prolongation, when compared to controls. Methods: A secondary analysis of the HF-ACTION dataset (n=2077) was performed, which randomized HFrEF (EF≤35%) patients to supervised AET compared to usual care . Patients were stratified by prolonged QRS (QRS interval ≥120ms). The association of QRS duration and survival from the primary outcome (all cause hospitalization or mortality) was assessed using Kaplan-Meier curves and univariable/multivariable Cox modeling using a backward stepwise approach. Results: Prolonged QRS participants were more likely to be older, white, and male. In univariable analyses, QRS prolongation was associated with increased risk of the primary outcome (HR 1.25, 95% CI [1.13, 1.39], p<0.001) whereas AET did not associate with differences in primary outcome (HR 0.93, 95% CI [0.84-1.04], p=0.2). Kaplan Meier curves stratified by QRS prolongation did not show a statistically significant relationship between AET and the primary outcome (Figure 1, 2). In multivariable analysis, QRS prolongation associated with increased risk of primary outcome (HR 1.20, 95% CI [1.07, 1.35], p=0.003), despite adjusting for cardiac resynchronization therapy (CRT) or implantable cardiac defibrillators (ICD); AET did not associate with a significant change in risk of primary outcome in the multivariable model (HR 0.95, 95% CI [0.85, 1.05], p=0.3). Discussion: Among ambulatory HFrEF patients, QRS prolongation was associated with increased risk of all-cause hospitalization or mortality. AET did not significantly influence risk of all-cause mortality or hospitalization, even after adjusting for CRT or ICD receipt. AET appears to be safe among patients with HFrEF and QRS prolongation. Few patients in this study had CRT placed; additional studies should investigate the effects of AET among patients with HFrEF and a CRT.
Chiang, Joey
(
University of Washington
, Seattle , Washington , United States )
Slocum, Charles
(
Seattle Children's Hospital
, Seattle , Washington , United States )
Li, Jason
(
University of Washington
, Seattle , Washington , United States )
Author Disclosures:
Joey Chiang:DO NOT have relevant financial relationships
| Charles Slocum:No Answer
| Jason Li:DO NOT have relevant financial relationships