Safety of Intracardiac Echocardiography Use in Transcatheter Aortic valve Replacement in comparison to Transesophageal Echocardiography: A National Inpatient Sample study
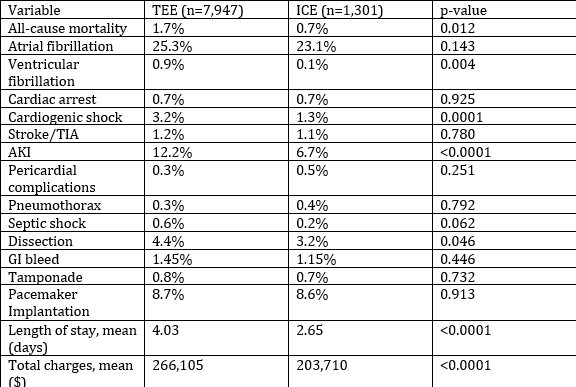
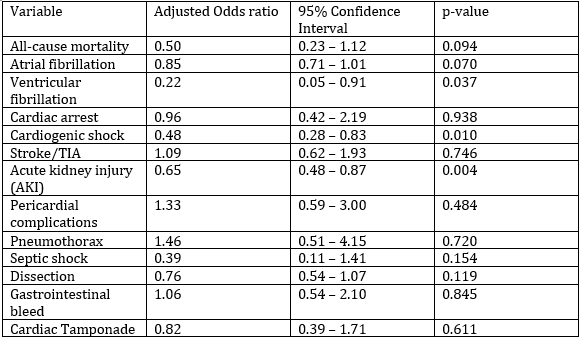
Abstract Body (Do not enter title and authors here): Introduction: Transesophageal echocardiography (TEE) has been widely used for imaging guidance during Transcatheter aortic valve replacement (TAVR) . However, the use of intracardiac echocardiography (ICE) is being recognized as a promising alternative imaging modality without the need for general anesthesia while providing high-resolution images. Real-world data on clinical outcomes comparing TEE- and ICE-directed TAVR remains limited. This study aimed to explore the in-hospital outcomes associated with ICE- versus TEE-guided TAVR using the US National Inpatient Sample (NIS). Methods: Using the NIS database from 2020 to 2022, we found adult patients who underwent TAVR with either TEE or ICE guidance. The possible confounders were adjusted through multivariable regression analyses. The evaluated outcomes included all-cause in-hospital mortality and complications such as atrial fibrillation, ventricular fibrillation, cardiogenic shock, acute kidney injury (AKI), stroke, and procedural complications. A p-value of <.05 was considered significant. Results: In a subpopulation of 9,248 patients, 85.9% (n=7,947) had TEE-guided and 14.1% (n=1,301) had ICE-guided TAVR. Majority of the population were males (57% vs 42%) and whites (87%) and the mean age group was 77 years. On unadjusted analysis, ICE-guided TAVR was associated with lower all-cause mortality (0.7% vs 1.7%, p=0.012), ventricular fibrillation (0.1% vs 0.9%, p=0.004), cardiogenic shock (1.3% vs 3.2%, p<0.0001), and AKI (6.7% vs 12.2%, p<0.0001). After adjustment, ICE-guided TAVR remained significantly associated with reduced odds of ventricular fibrillation (adjusted OR 0.22; 95% CI: 0.05–0.91; p=0.037), cardiogenic shock (aOR 0.48; 95% CI: 0.28–0.83; p=0.01), and AKI (aOR 0.65; 95% CI: 0.48–0.87; p=0.004) while the periprocedural complication rates including pericarditis, pericardial effusion and tamponade, pneumothorax, dissection and pacemaker implantation remained similar in both the groups. The ICE group had a mean length of stay that was 1.38 days shorter (2.65 vs 4.03 days, p<0.001), and the total hospitalization cost was significantly lower by $57,595 (ICE: $203,710 vs TEE: $266,105; p<0.001). Conclusions: ICE-guided TAVR was associated with favorable in-hospital outcomes, reflecting lower rates of ventricular fibrillation, cardiogenic shock, and AKI, as well as significantly shorter hospital stays and reduced costs, compared to TEE-guided TAVR.
Perumalla, Hima Sanjana
(
University of Missouri Kansas City
, Kansas city , Missouri , United States )
Jain, Samiksha
(
Guntur Medical College
, Guntur , India )
Khan, Abdul Wali
(
University of Missouri Kansas City
, Kansas City , Missouri , United States )
Modi, Karnav
(
University of Missouri Kansas City
, Kansas City , Missouri , United States )
Jitta, Sahas Reddy
(
Mercy Hospital
, Maryland heights , Missouri , United States )
El Mais, Huda
(
St. Luke's MAHI - UMKC
, Kansas City , Missouri , United States )
Lingamsetty, Shanmukh Sai Pavan
(
Mamata Medical College
, Khammam , India )
Asif, Talal
(
Saint Luke's Mid America Heart Inst
, Kansas City , Missouri , United States )
Author Disclosures:
Hima sanjana Perumalla:DO NOT have relevant financial relationships
| Samiksha Jain:DO NOT have relevant financial relationships
| Abdul Wali Khan:DO NOT have relevant financial relationships
| Karnav Modi:DO NOT have relevant financial relationships
| Sahas Reddy Jitta:DO NOT have relevant financial relationships
| Huda El Mais:DO NOT have relevant financial relationships
| Shanmukh sai pavan Lingamsetty:DO NOT have relevant financial relationships
| TALAL ASIF:DO NOT have relevant financial relationships