Efficacy and Safety of Oral Anticoagulant Monotherapy vs. Dual Therapy in Atrial Fibrillation with Stable Coronary Artery Disease: A Systematic Review and Meta-Analysis
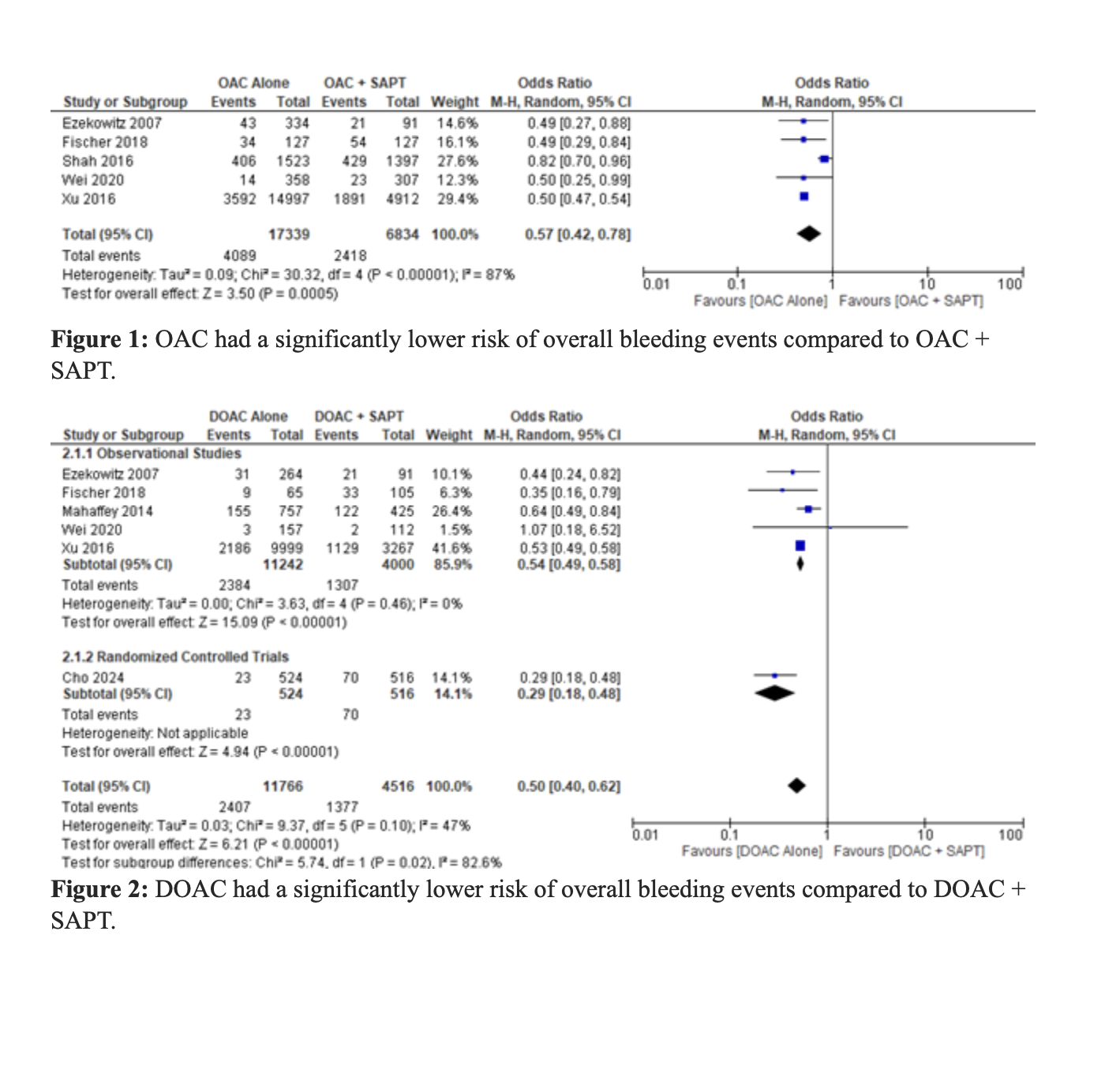
Abstract Body (Do not enter title and authors here): Introduction: In patients with atrial fibrillation (AF) and stable ischemic heart disease, guidelines currently recommend oral anticoagulant (OAC) monotherapy over combination therapy with OAC and a single antiplatelet agent (SAPT). However, the comparative safety and efficacy of these strategies remain under-investigated. Methods: We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) and observational studies comparing OAC monotherapy to OAC + SAPT in patients with nonvalvular AF and stable CAD. Databases searched included PubMed, Google Scholar, Cochrane Library, Embase, Scopus, Web of Science, and ClinicalTrials.gov. Outcomes assessed were all-cause mortality, cardiovascular mortality, major adverse cardiac events (MACE), myocardial infarction (MI), stroke (ischemic and hemorrhagic), and various bleeding events. Results: Twenty-three studies (3 RCTs, 20 observational), encompassing 51,396 patients (mean age 72.5 years, mean follow-up 4.8 years), were included. OAC monotherapy was associated with a significantly lower risk of overall bleeding compared to OAC + SAPT (OR 0.57, 95% CI 0.42–0.78; P=0.0005). DOAC monotherapy also significantly reduced the risk of overall bleeding compared to DOAC + SAPT [OR 0.50, 95% CI 0.40–0.62; P < 0.00001]. Among DOACs, apixaban provided the greatest reduction in overall bleeding events [OR 0.35, 95% CI 0.16–0.79; P=0.01]. OAC monotherapy was similarly effective in reducing the risk of major bleeding events compared to OAC + SAPT [OR 0.64, 95% CI 0.59–0.69; P < 0.00001], with DOACs showing a comparable benefit [OR 0.61, 95% CI 0.48–0.78; P < 0.0001]. Edoxaban showed the greatest reduction in major bleeding risk [OR 0.45, 95% CI 0.21–0.96; P=0.04]. OAC monotherapy also significantly reduced gastrointestinal bleeding (OR 0.61, P=0.003) and MI (OR 0.86, P=0.004), with edoxaban again demonstrating the greatest MI reduction (OR 0.67, P=0.004).While reductions in MACE were borderline significant (OR 0.82, P=0.02), DOAC monotherapy showed a similar trend (OR 0.71, P=0.03). There were no significant differences in all-cause or cardiovascular mortality, or stroke outcomes, between OAC monotherapy and combination therapy. Conclusion: OAC monotherapy offers superior bleeding and MI risk reduction compared to OAC + SAPT in patients with AF and stable CAD, with no increased risk of mortality or stroke. These findings support current guideline recommendations favoring OAC monotherapy in this population.
Sabri, Muhammad
(
Abington Jefferson Hospital
, Horsham , Pennsylvania , United States )
Al Hennawi, Hussam
(
Jefferson Abington Hospital
, Willow Grove , Pennsylvania , United States )
Khan, Muhammad Khuzzaim
(
DOW
, KARACHI , Pakistan )
Duseja, Nikhil
(
Karachi Medical and Dental College
, KARACHI , Pakistan )
Nair, Abhinav
(
Abington Jefferson Hospital
, Horsham , Pennsylvania , United States )
Author Disclosures:
Muhammad Sabri:DO NOT have relevant financial relationships
| Hussam Al Hennawi:No Answer
| Muhammad Khuzzaim Khan:DO NOT have relevant financial relationships
| Nikhil Duseja:DO NOT have relevant financial relationships
| Abhinav Nair:No Answer