Dual Pathway Inhibition prescription after percutaneous vascular intervention is low, and dependent on physician and treating facility practice patterns
Abstract Body (Do not enter title and authors here): Introduction: Industry-funded level one data supports dual pathway inhibition (DPI; aspirin and low-dose rivaroxaban) after percutaneous vascular interventions (PVI), but interventionalists debate its widespread adoption.
Research Questions: What are the rates of and factors associated with pre and post-PVI DPI prescription in the Vascular Quality Initiative (VQI)?
Methods: We queried the VQI for PVI (2022-2024), excluding acute limb ischemia, aneurysmal disease, COVID+ patients, and those on full dose anticoagulation. DPI was defined as any antiplatelet therapy plus 2.5mg twice daily of rivaroxaban. Mann-Kendal tests evaluated pre- and post-PVI antithrombotic prescription trends. Mixed-effects logistic regression modeled factors associated with pre- and post-PVI DPI prescription, clustered by physician and treating facility, to evaluate the influence of provider and practice-level variation beyond patient characteristics.
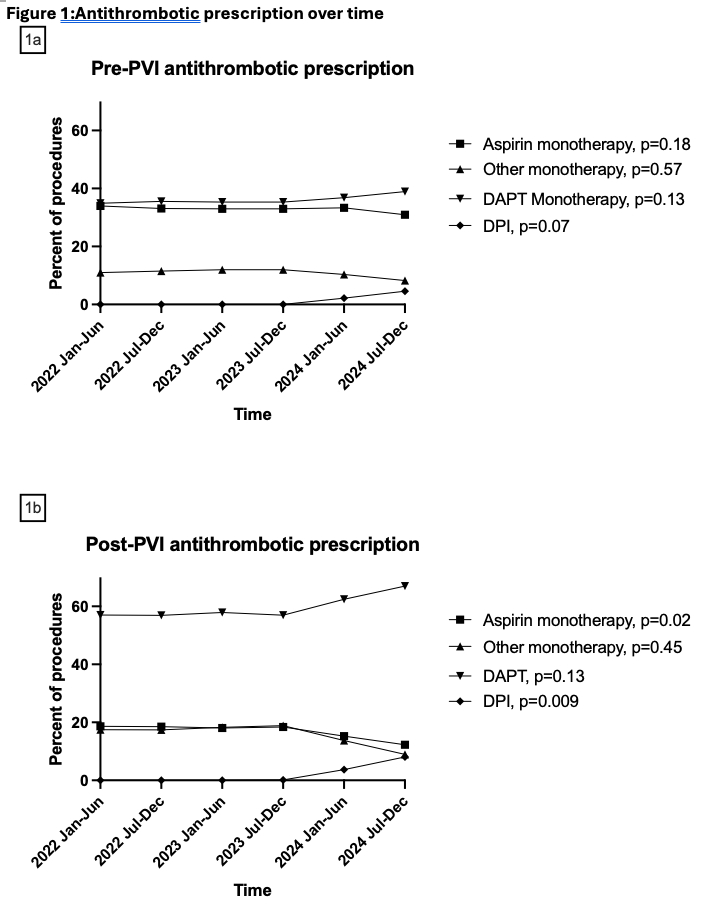
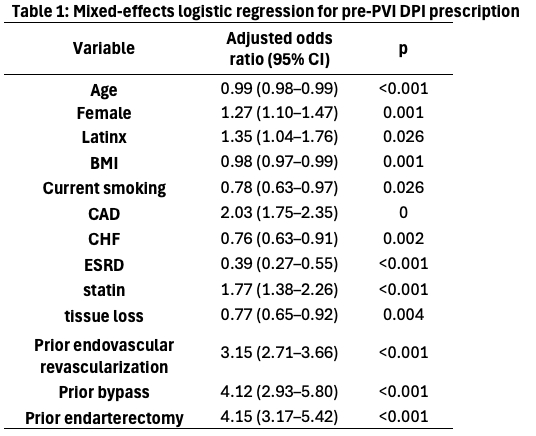
Results: There were no significant changes in pre-PVI prescription patterns over the study period. DPI prescription increased non-significantly from 0/20,058 (0%) in early 2022 to 434/9,488 (4.6%) in late 2024 (Figure 1a). Female sex, Latinx ethnicity, CAD, statin, and prior revascularization were associated with increased pre-PVI DPI prescription. Increasing age and BMI, CHF, ESRD, current smoking, and tissue loss were negatively associated with pre-PVI DPI prescription (Table 1). Physician accounted for 17.4% of variation in pre-PVI DPI prescribing, while treating facility accounted for 14.4% for a total of 31.8%.
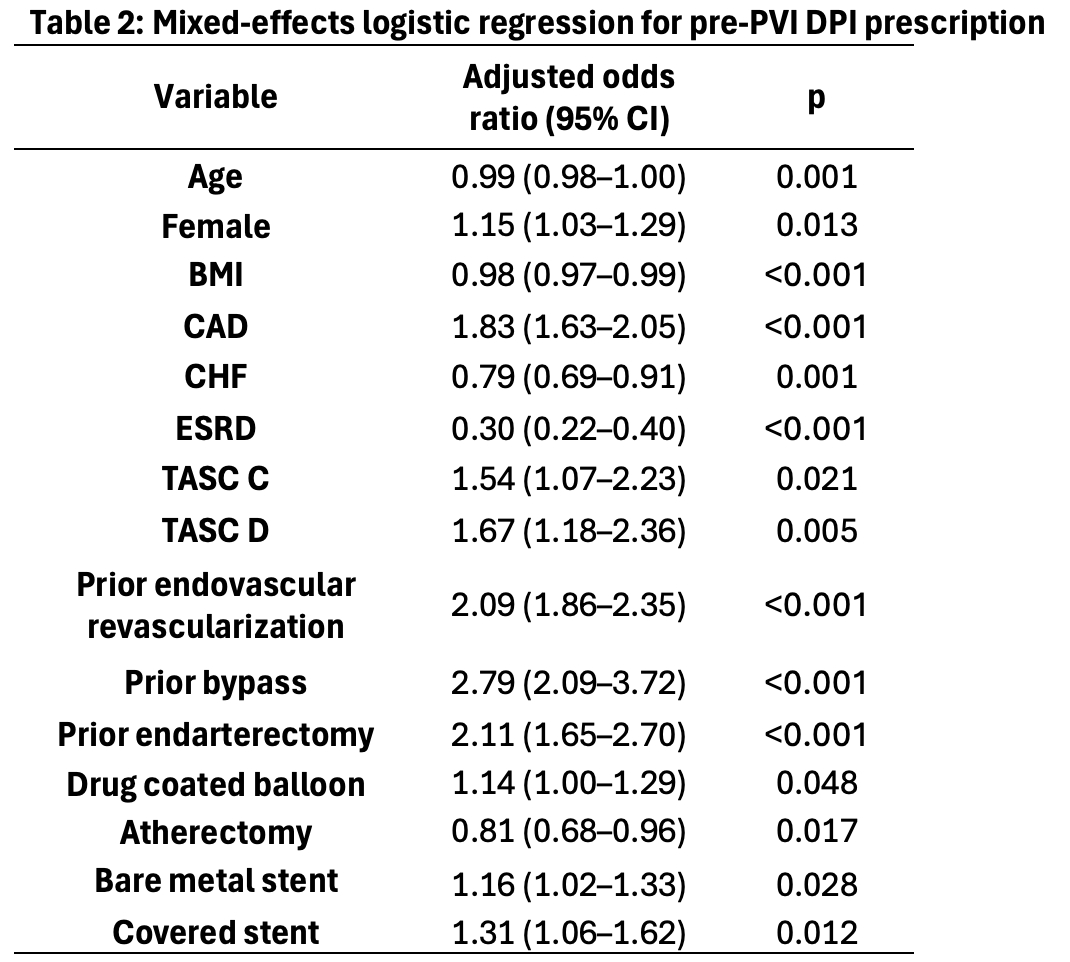
Post-PVI DPI prescription increased significantly over the study period from 0/20,075 (0%) in early 2022 to 742/9,200 (8.1%) in late 2024. Aspirin monotherapy decreased significantly (Figure 1b). Female sex, CAD, increased Trans-Atlantic Inter-Society Consensus (TASC) score, prior revascularization, drug coated balloon, and stent placement were associated with increased post-PVI DPI prescription. Increasing age and BMI, CHF, ESRD, and atherectomy were negatively associated with DPI prescription (Table 2). Physician accounted for 22.0% of variation in post-PVI DPI prescribing, whereas treating facility accounted for 12.6% for a total of 34.6%.
Conclusions: Pre and post-PVI DPI prescription was low in our cohort, although did increase significantly to 8.1% post-PVI during the study period. Physician and treating facility practice patterns accounted for one third of the variation in DPI prescribing.
Jarosinski, Marissa
(
UPMC
, Pittsburgh , Pennsylvania , United States )
Lowenkamp, Mikayla
(
UPMC
, Pittsburgh , Pennsylvania , United States )
Madigan, Michael
(
UPMC
, Pittsburgh , Pennsylvania , United States )
Reitz, Katherine
(
UPMC
, Pittsburgh , Pennsylvania , United States )
Chaer, Rabih
(
UPMC
, Pittsburgh , Pennsylvania , United States )
Sridharan, Natalie
(
UPMC
, Pittsburgh , Pennsylvania , United States )
Author Disclosures:
Marissa Jarosinski:DO NOT have relevant financial relationships
| Mikayla Lowenkamp:DO NOT have relevant financial relationships
| Michael Madigan:DO NOT have relevant financial relationships
| Katherine Reitz:No Answer
| Rabih Chaer:No Answer
| Natalie Sridharan:DO NOT have relevant financial relationships