Scientific Sessions 2025
/
Advances in Venous Thromboembolic Disease
/
Utilization trends and outcomes of mechanical thrombectomy, catheter directed thrombolysis and systemic thrombolysis in patients with massive and submassive pulmonary embolism. An analysis of the National Inpatient Sample Database from 2017 to 2021
American Heart Association
105
0
Final ID: MP2594
Utilization trends and outcomes of mechanical thrombectomy, catheter directed thrombolysis and systemic thrombolysis in patients with massive and submassive pulmonary embolism. An analysis of the National Inpatient Sample Database from 2017 to 2021
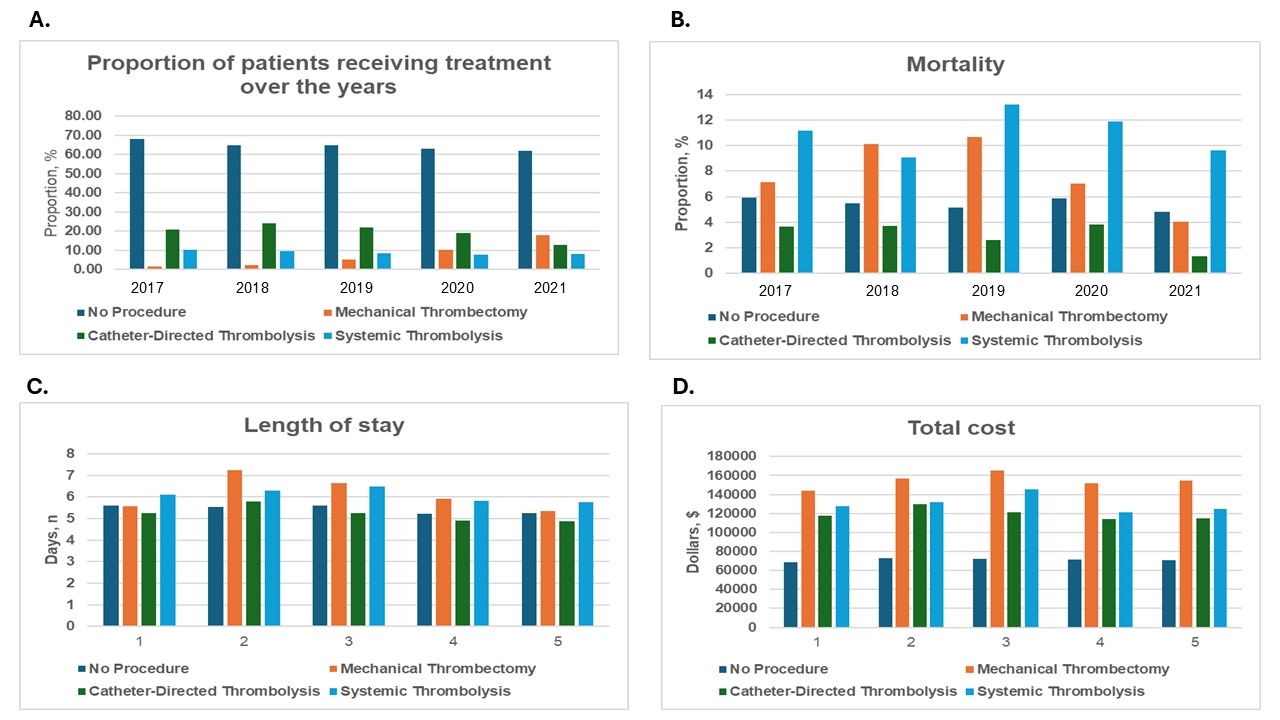
Abstract Body (Do not enter title and authors here): Introduction: Pulmonary embolism (PE) is associated with cardiovascular mortality, especially in massive and submassive casese requiring urgent intervention. Approximately 10% of symptomatic PEs are rapidly fatal. Given the bleeding risk associated with systemic thrombolysis (ST), catheter-directed thrombolysis (CDT) and mechanical thrombectomy (MT) have emerged as alternative treatments. Objectives. To evaluate trends in the utilization of and mortality associated with ST, CDT and MT. Methods. Using the National Inpatient Sample database (2017-2021), patients with massive and submassive PE were identified using validated ICD-10 codes, along with corresponding procedure codes for ST, CDT and MT. Trends in incidence, mortality, length of stay (LOS) and hospital costs were analyzed. Logistic regression was used to assess differences in outcomes over five years. Results. The number of patients diagnosed with massive and submassive PE increased from 13,265 in 2017 to 23,075 in 2021. While utilization of MT rose over the years (1.58% in 2017 to 17.70% in 2021), ST utilization initial declined until 2019, followed by a plateu over the subsequent two years. CDT utilization peaked in 2018 (23.94%), before declining to 12.92% in 2021. Overall, there was a borderline significant reduction in mortality (OR, 0.96; 95% CI, 0.91- 1.003; P=0.06), a significant reduction in the LOS (P <0.0001), and increase in hospital costs (P=0.018) over the five-year period. In the MT subgroup, there was a significant reduction in mortality (OR, 0.77; 95% CI, 0.67- 0.88; P <0.0001), and LOS (P=0.021), without a significant change in total costs (P=0.34). The CDT subgroup demonstrated reduced LOS (P= 0.002) and total costs (P=0.041), but unchanged mortality. The ST sungroup showed no differences in mortality, LOS or total costs. Overall, there was no significant differences in mortality, LOS or total costs between the three groups. Discussion. Increased utilization of MT along with reductions in mortality likely reflect advancements in device safety and efficacy. Reduced utilization of ST and CDT, without corrsponding improvements in mortality may reflect bleeding concerns. These findings suggest a shift towards MT utilization, warranting further research on long-term safety and efficacy.
Nandyal, Shreyas
(
Cook County Health
, Chicago , Illinois , United States )
Varma, Revati
(
Cook County Health
, Chicago , Illinois , United States )
Odoi, Samuel
(
Cook County Health
, Chicago , Illinois , United States )
Gajjar, Rohan
(
Cook County Health
, Chicago , Illinois , United States )
Nissan, Ninos
(
Cook County Health
, Chicago , Illinois , United States )
Author Disclosures:
Shreyas Nandyal:DO NOT have relevant financial relationships
| Revati Varma:DO NOT have relevant financial relationships
| Samuel Odoi:DO NOT have relevant financial relationships
| Rohan Gajjar:No Answer
| Ninos Nissan:DO NOT have relevant financial relationships