QT Interval Prolongation Is Independently Associated With Hypermagnesemia: Insights From A Single-Center Observational Study
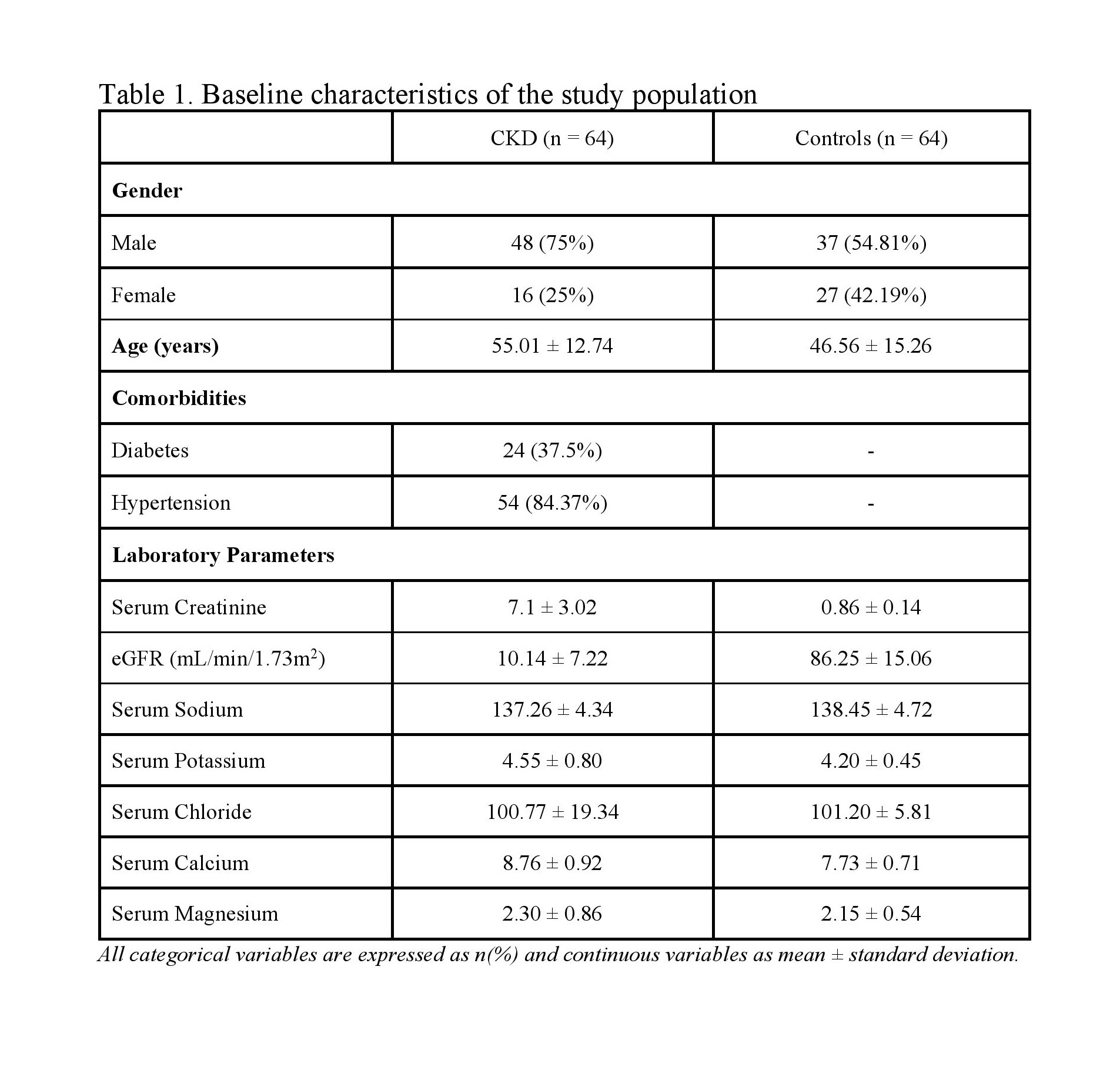
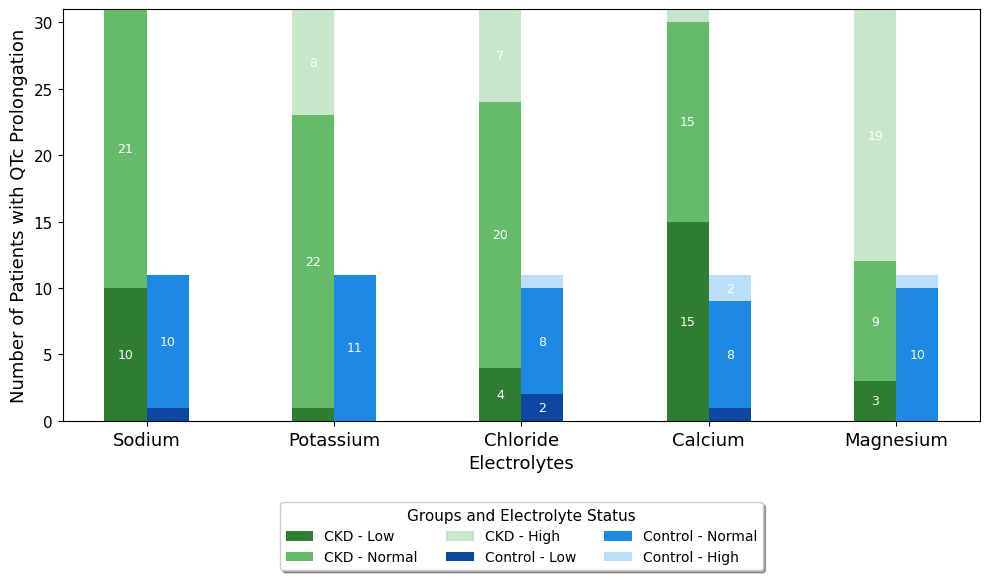
Abstract Body (Do not enter title and authors here): Introduction: Ventricular arrhythmias and sudden cardiac death are among the leading causes of mortality in patients with chronic kidney disease (CKD). This risk arises from shared etiologies between CKD and cardiovascular disease, including diabetes, hypertension, aging, and electrolyte imbalances. QT prolongation is a hallmark of ventricular arrhythmias often influenced by electrolyte disturbances in CKD. While previous studies have described QT prolongation in CKD, the role of electrolyte abnormalities remains unclear. Aims: We aimed to assess the prevalence of QT prolongation in CKD patients compared to controls and evaluate its association with serum electrolytes and renal function. Methods: A cross-sectional study was conducted over two months at a tertiary care center in south India. Adults ≥18 years who met the eGFR or imaging criteria for CKD were included. Exclusion criteria were ischemic heart disease, left ventricular hypertrophy, bundle branch blocks, LVEF ≤55%, and use of QT-prolonging medications. QT interval corrected for heart rate (QTc) was measured and prolongation was defined as ≥450 ms (males) and ≥460 ms (females). Serum electrolytes (Na+, K+, Ca2+, Mg2+, Cl-) were measured, and eGFR was calculated using CKD-EPI equation. Multivariable logistic regression identified independent predictors of QTc prolongation, adjusted for age, sex, eGFR, and magnesium. Results: A total of 64 CKD patients and 64 controls were included. QTc prolongation was more common in CKD patients than controls (48.4% vs 16.9%). Those with QTc prolongation were younger (49 ± 13.3 vs 51.7 ± 15.2 years) and had lower eGFR (26.3 vs 60.2 mL/min/1.73m2). Hypermagnesemia was more prevalent in patients with QTc prolongation in the CKD cohort (p=0.01), and normal magnesium status was independently associated with lower odds of QTc prolongation (OR 0.22, p=0.01). QTc correlated positively with serum Cl- (r= -0.25, p<0.05) and negatively with eGFR (r=-0.27, p<0.05). Lower eGFR was marginally significant as a predictor of QTc prolongation (OR 0.88, p=0.05). Mean QTc did not differ across CKD stages (p>0.05). Conclusion: QTc prolongation is more prevalent in CKD and correlates with declining renal function. Hypermagnesemia emerged as an independent, modifiable predictor. These findings underscore the need for routine QTc and electrolyte monitoring to reduce arrhythmia risk in CKD.
Murali, Mathangi
(
Government Erode Medical College
, Erode , India )
Veeraraghavan, Kanchana
(
Private Practitioner
, Erode , India )
Author Disclosures:
Mathangi Murali:DO NOT have relevant financial relationships
| Kanchana Veeraraghavan:No Answer