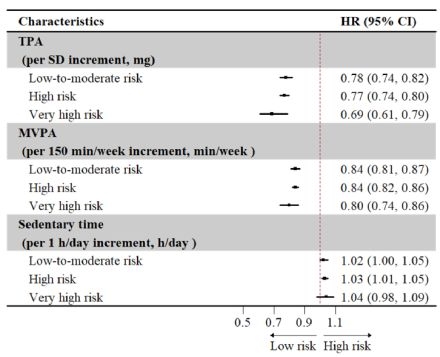
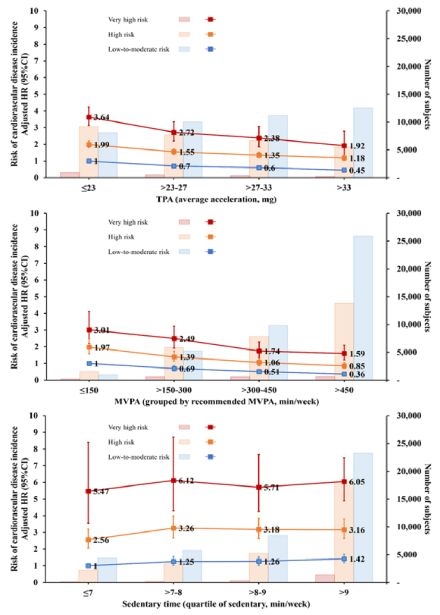
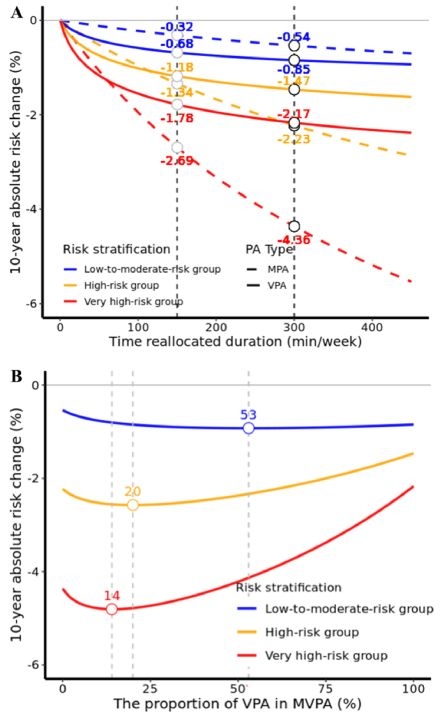
Abstract Body (Do not enter title and authors here): Introduction: The “one-size-fits-all” recommendations in current physical activity (PA) guidelines have been challenged, and optimal PA patterns across individuals with varying predicted cardiovascular disease (CVD) risk remain unclear. Methods: We analyzed 72 884 UK Biobank participants (mean [SD] age, 56.0 [7.8] years; 57.1% female), with total volume of PA (TPA), moderate-intensity PA (MPA), vigorous-intensity PA (VPA), moderate-to-vigorous-intensity PA (MVPA), and sedentary time assessed by accelerometers. Participants were divided into low-to-moderate-, high-, or very high-risk groups by the updated Systemic Coronary Risk Estimation 2 (SCORE2), SCORE2-Older Persons, and SCORE2-Diabetes algorithms. Cox regression and compositional data analysis were used to estimate the association between PA and incident CVD events and the potential benefit of reallocating sedentary time to MVPA. Results: A total of 5695 incident CVD events occurred. Higher TPA and MVPA were associated with lower CVD risk, and the association was most pronounced among those from the very high-risk group (Figures 1 and 2). For example, the hazard ratio (HR) was 0.80 (95% CI, 0.74-0.86), 0.84 (0.82-0.86) and 0.84 (0.81-0.87) per 1-SD increase in MVPA for individuals with very-high, high and low-to-moderate risk, respectively (Pinteraction<0.001). In addition, individuals may benefit more from allocating sedentary time to active PA with the increased predicted CVD risk (Figure 3A). Further analyses revealed that current recommendations from PA guidelines (150-300 min/week of MPA or 75-150 min/week of VPA [or an equivalent combination]) should be refined according to individuals’ risk stratification. In low-to-moderate-risk individuals, any guideline-recommended combinations of MPA and VPA were beneficial. In high-risk individuals, VPA exceeding 60 min/week may attenuate benefits, while in very high-risk individuals, optimal benefits were observed at 42 min/week of VPA, beyond which benefits may decline (Figure 3B). Conclusions: Optimal PA pattern for cardiovascular health significantly varied across individuals at different risk, and the optimal VPA threshold should be underscored, especially for high- or very high-risk groups. This study calls for personalized PA recommendations by integrating risk assessment, and provides evidence for promoting the guidelines towards a more comprehensive and individualized development.
Yuan, Chenxi
(
Fuwai Hospital
, Beijing , China )
Zhou, Tao
(
Fuwai Hospital
, Beijing , China )
Cui, Xiang
(
Fuwai Hospital
, Beijing , China )
Xie, Shaohua
(
Karolinska Institutet
, Stockholm , Sweden )
Lu, Xiangfeng
(
Fuwai Hospital
, Beijing , China )
Liu, Fangchao
(
Fuwai Hospital
, Beijing , China )
Author Disclosures:
Chenxi Yuan:No Answer
| Tao Zhou:DO NOT have relevant financial relationships
| Xiang Cui:No Answer
| Shaohua Xie:No Answer
| Xiangfeng Lu:No Answer
| fangchao liu:DO NOT have relevant financial relationships
Jiang Chao, Dong Jianzeng, Cai Jun, Anderson Craig, Du Xin, Tang Yangyang, Han Rong, Song Yanna, Wang Chi, Lin Xiaolei, Yi Yang, Rodgers Anthony, Ma Changsheng
Liu Fangchao, Yu Ling, Lin Jinchun, Lu Xiangfeng, Huang Jianfeng, Gu Dongfeng, Chen Shufeng, Liang Fengchao, Li Jianxin, Huang Keyong, Sun Yingxian, Wang Qing, Wu Shouling, Ma Mingfeng