Peripheral Artery Disease and Post-Transplant Outcomes: Disease Burden Overcomes Distribution
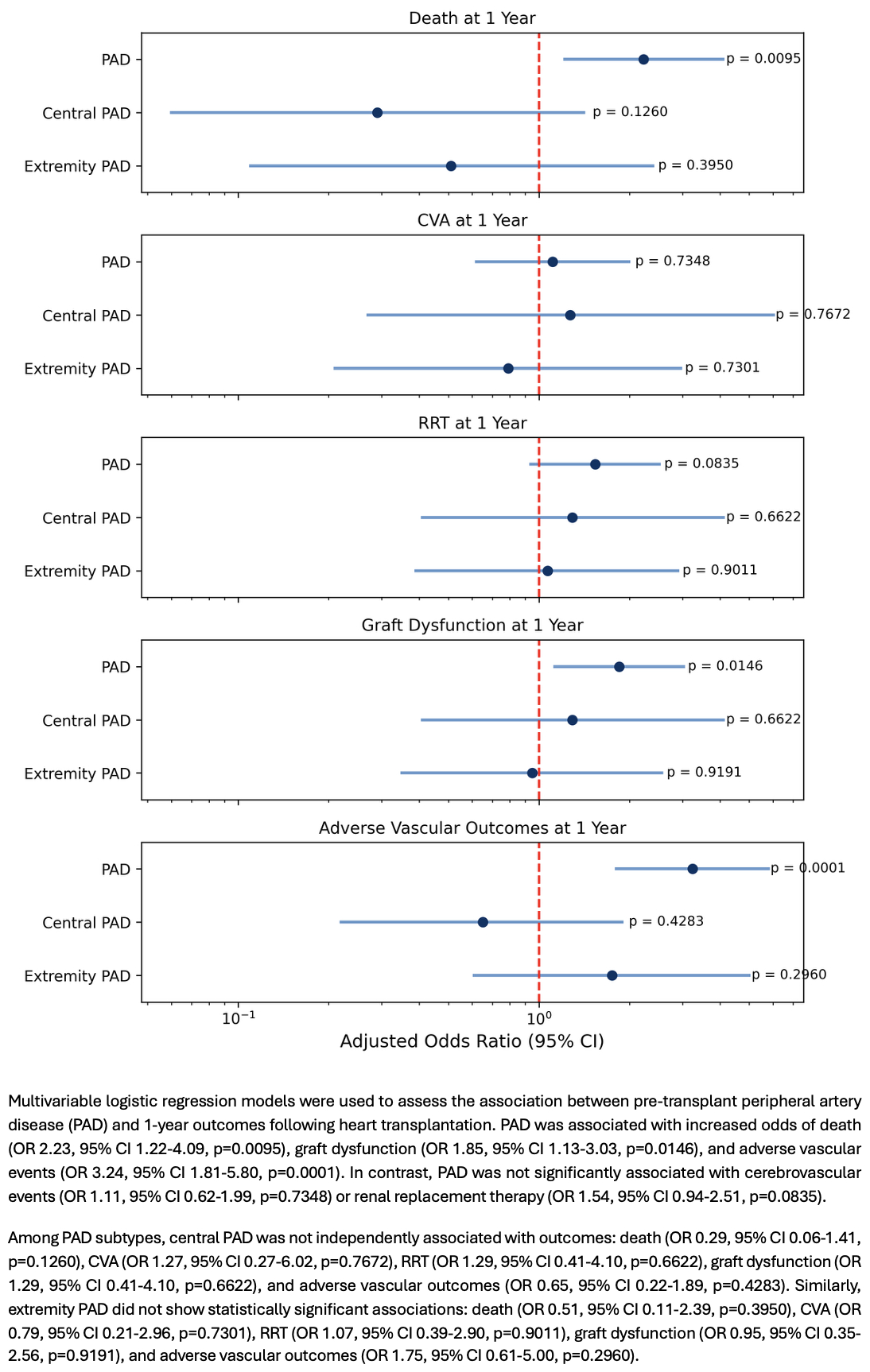
Abstract Body (Do not enter title and authors here): Introduction: Peripheral artery disease (PAD) is a known risk factor for adverse cardiovascular outcomes and has historically been viewed as a relative contraindication to heart transplantation (HT). However, as management of PAD improves and transplant eligibility broadens, the impact of PAD on post-HT outcomes warrants reevaluation. Hypothesis: Pre-HT PAD, driven by extremity PAD, is associated with increased risk of 1-year post-HT adverse outcomes, including all-cause mortality, cerebrovascular accident (CVA), renal replacement therapy (RRT), graft dysfunction, and adverse vascular outcomes. Methods: We conducted a retrospective cohort study of patients who underwent HT at a large, advanced heart failure center from January 2012 to May 2022. PAD was defined by history of CVA, claudication, abnormal ankle-brachial index (ABI <1), abnormal carotid dopplers (>50% stenosis), or abnormal upper or lower extremity arterial dopplers (>50% stenosis). Patients were stratified by PAD status and subtype: central/cerebrovascular (CVA or abnormal carotid dopplers) and extremity (claudication, abnormal ABI, or abnormal extremity dopplers). Outcomes included 1-year all-cause mortality, CVA, RRT, graft dysfunction (ejection fraction <55%), and vascular complications (consults or abnormal imaging). Group comparisons used multivariable logistic regression adjusted for PAD subtype using Python®. Results: Of the 595 patients (mean age 53 years; 28% female; 27% Black), 216 (36%) had PAD. The PAD group exhibited higher rates of pre-HT diabetes (32% vs 21%, p<0.01) and hypertension (58% vs 44%, p<0.01). No significant differences in age, sex, race, kidney disease, or smoking were found between groups. In the PAD group, one-year all-cause mortality was more than double those without PAD (11.6% vs 5.5%, p=0.01). Graft dysfunction was also higher (16.7% vs 9.8%, p=0.02), while CVA (9.3% vs 8.4%, p=0.85) and RRT (15.7% vs 10.8%, p=0.11) were not significantly different in PAD patients compared to those without. PAD patients also had increased vascular complications at 1 year (15.3% vs 5.3%, p<0.001). However, when stratified by PAD subtype, neither central/cerebrovascular nor extremity PAD independently predicted outcomes (Figure). Conclusion: Total PAD burden pre-HT was associated with increased all-cause mortality, graft dysfunction, and vascular complications at 1 year. These findings underscore the importance of incorporating PAD into pre- and post-HT management.
Hadid, Bana
(
Columbia University Medical Center
, New York , New York , United States )
Mantini, Devin
(
Columbia University Medical Center
, New York , New York , United States )
Schwartz, Sarah
(
Columbia University Medical Center
, New York , New York , United States )
Labarre, Brian
(
Columbia University Medical Center
, New York , New York , United States )
Uriel, Nir
(
Columbia University Medical Center
, New York , New York , United States )
Sayer, Gabriel
(
Columbia University Medical Center
, New York , New York , United States )
Author Disclosures:
Bana Hadid:DO NOT have relevant financial relationships
| Devin Mantini:No Answer
| Sarah Schwartz:DO NOT have relevant financial relationships
| Brian LaBarre:No Answer
| Nir Uriel:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Abbott:Active (exists now)
; Research Funding (PI or named investigator):Fire 1:Active (exists now)
; Research Funding (PI or named investigator):Abiomed:Active (exists now)
| Gabriel Sayer:DO have relevant financial relationships
;
Consultant:Abbott:Active (exists now)
; Consultant:Thermo Fisher Science:Active (exists now)