Risk Stratification Model on Mortality in Vulnerable Patients with Chronic Limb-Threatening Ischemia
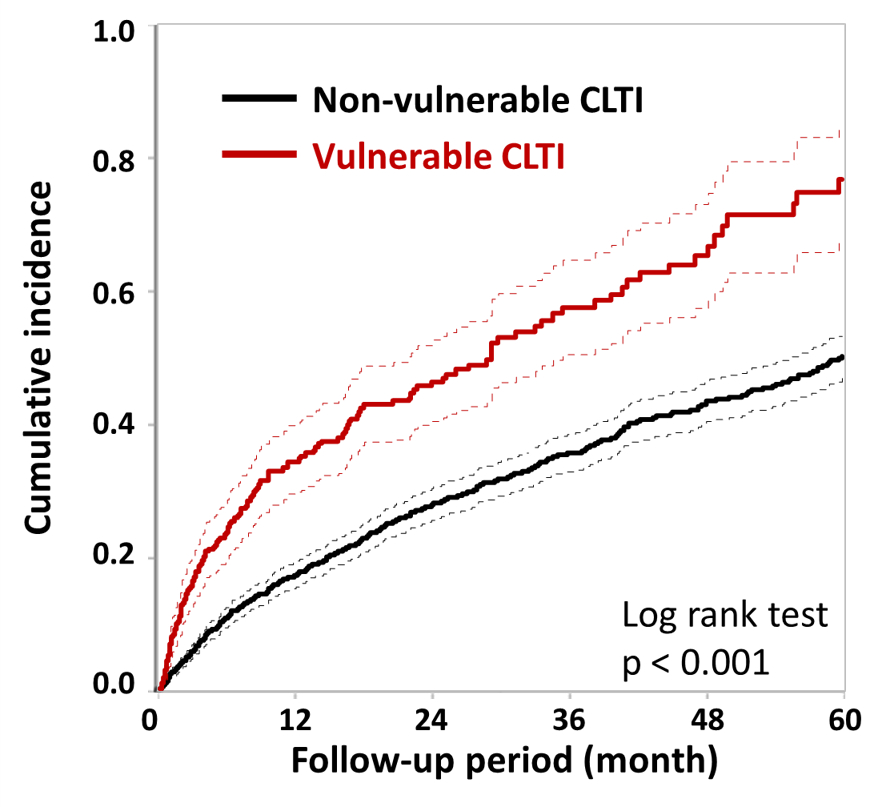
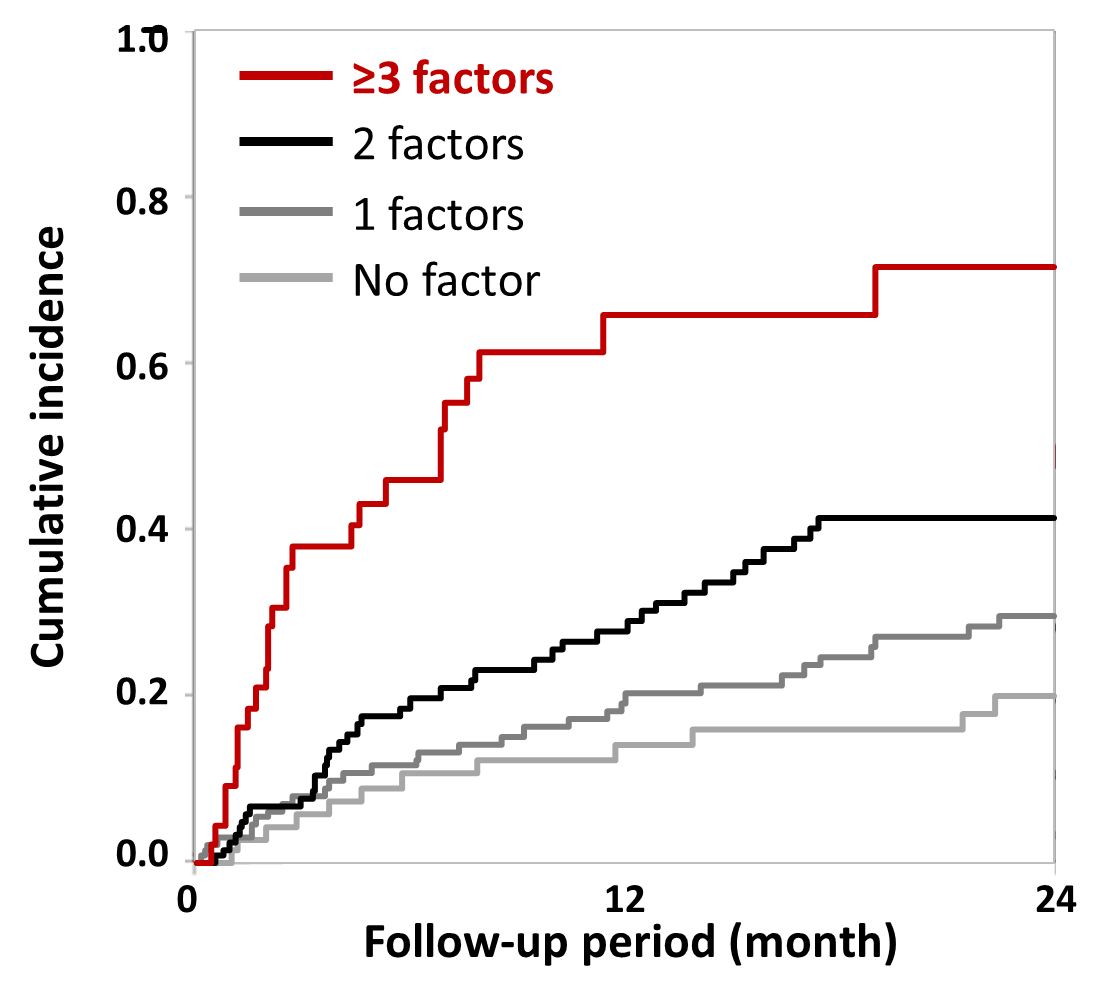
Abstract Body (Do not enter title and authors here): Background: The prevalence of peripheral arterial disease, including chronic limb-threatening ischemia (CLTI), is globally increasing due to the aging society and the pandemics of diabetes mellitus. Although managing elderly CLTI patients with non-ambulatory status is substantially common in clinical practice, determination of treatment planning remains clinically challenging. This study aimed to evaluate the mortality and prognostic factors in elderly CLTI patients with non-ambulatory. Methods: This was a multicenter retrospective observational study enrolling 2309 CLTI patients (age: 75.5 ± 10.2 years, male: 60.5%, diabetes mellitus: 61.9%, dialysis: 46.9%) who underwent endovascular therapy (EVT) between April 2010 and March 2024. Patients aged over 80 years old with non-ambulatory status including wheelchair or bedridden were defined as the vulnerable CLTI group. The primary outcome measure was all-cause mortality, and were analyzed by multivariate analysis. Results: A total of 443 patients (19.2%) were classified as vulnerable CLTI. The 5-year all-cause mortality rate was 76.4% in the vulnerable CLTI group and 49.9% in the non-vulnerable CLTI group (p<0.001). The multivariate analysis revealed hemodialysis (hazard ratio [HR]: 1.83, p < 0.001), wound, ischemia, and foot infection (WIfI) stage 4 (HR: 1.71, p = 0.002), left ventricular ejection fraction < 50% (HR: 1.52, p = 0.04), and serum albumin level < 3 g/dL (HR: 1.55, p = 0.009) were positively associated with mortality in vulnerable CLTI group, with no significant interactions. 12-month mortality rate was 71.6% in patients with three or more of these risk factors. Conclusions: The current study revealed that hemodialysis, wound severity, malnutrition, and cardiac dysfunction were significantly associated with mortality in vulnerable CLTI patients. Risk stratification based on these predictors allows estimation of prognosis in vulnerable CLTI patients, and would be clinically useful for determination of treatment planning including palliative care.