Sex-related differences in clinical outcomes among heart failure patients with cardiac amyloidosis on SGLT2i therapy
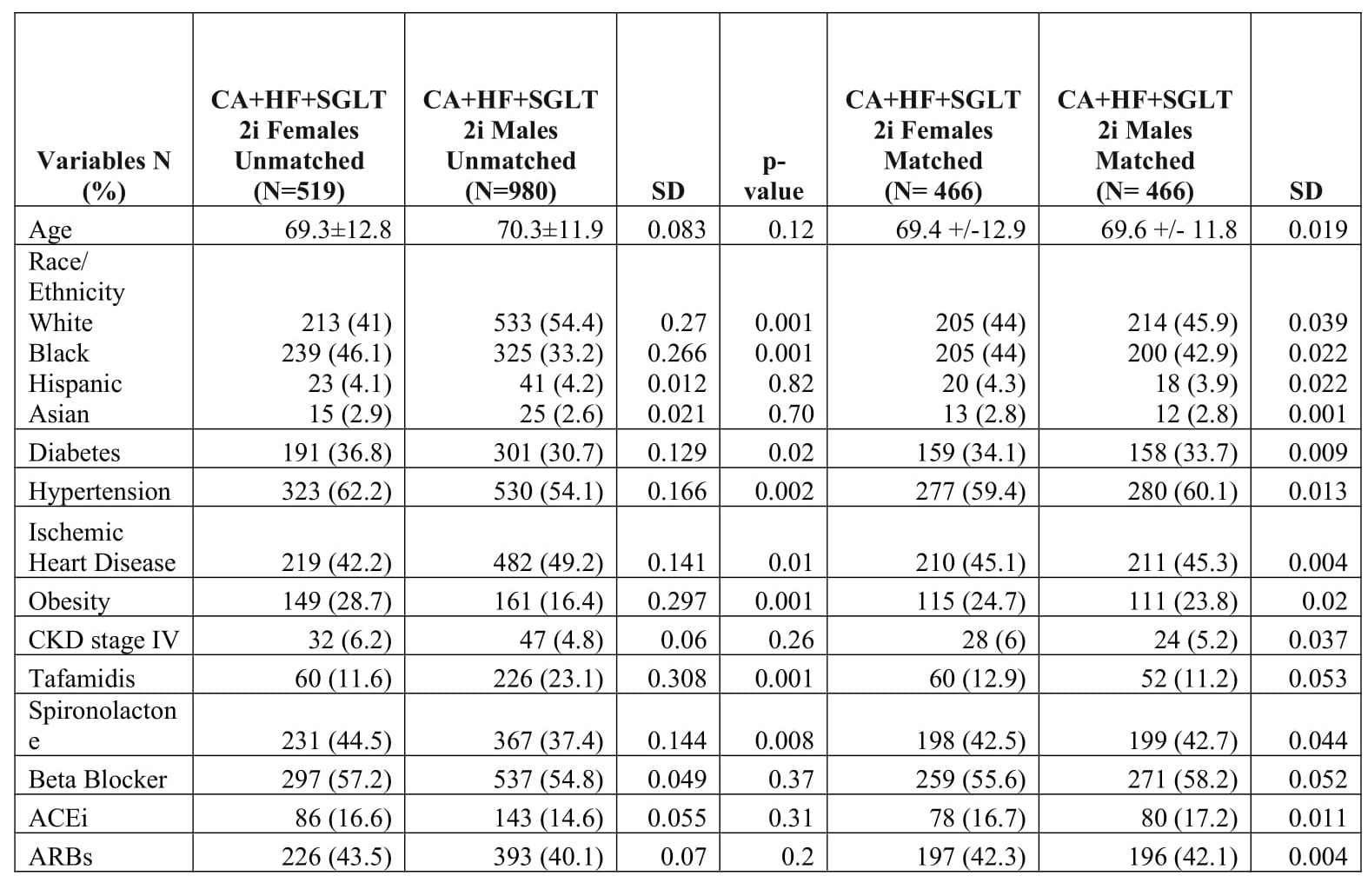
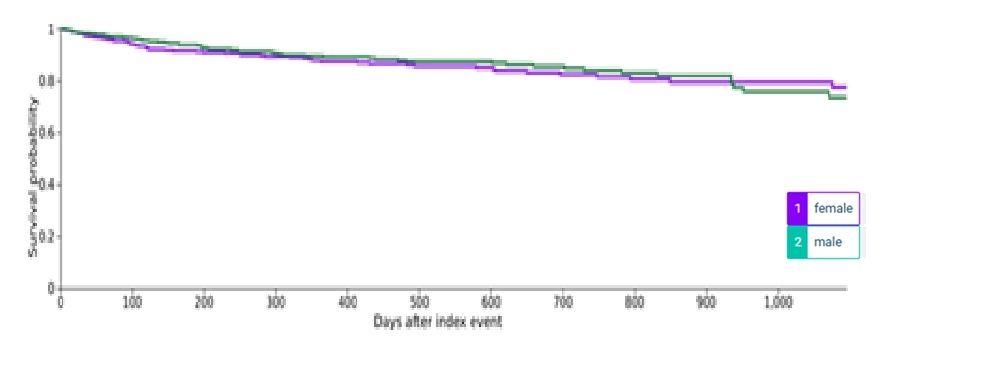
Abstract Body (Do not enter title and authors here): Background: Sodium-glucose cotransporter-2 inhibitors (SGLT2i) have shown morbidity and mortality benefits in patients with heart failure (HF) and cardiac amyloidosis (CA). CA accounts for ~15% of HFpEF cases—a condition that is twice as prevalent in females compared to males. Despite growing recognition of CA and its early presentation as HFpEF, data on SGLT2i use and outcomes in females with CA and HF remain limited. We evaluated sex-based differences in outcomes in this population. Methods: A retrospective study using TriNetX platform included patients ≥18 years with CA and HF on SGLT2i therapy, identified using ICD-10 codes. Patients were grouped by sex and baseline characteristics, including demography, medications, and comorbid conditions (ischemic heart disease [IHD], hypertension, diabetes mellitus type 2 [DM], obesity, chronic kidney disease [CKD] stages I-IV, peripheral vascular disease, smoking, and alcohol history) were assessed 6 months before initiating SGLT2i. Exclusions included CKD stage V, end-stage renal disease (ESRD), type 1 DM, history of diabetic ketoacidosis, and atrial fibrillation. Propensity score matching (PSM) (1:1, SD<0.1) balanced the baseline characteristics. Cox regression and Kaplan–Meier survival curves evaluated clinical outcomes at 6 months and 3 years. Results: Of 13,127 patients with HF and CA, only 11.4% were prescribed SGLT2i. Despite comprising 44% of the CA and HF cohort, females accounted for only 34.6% of SGLT2i users, compared to 65.4% of males. Compared to males, females had a significantly higher proportion of Blacks, DM, hypertension, obesity, and spironolactone use. In contrast, males had a significantly higher proportion of Whites, IHD, and tafamidis use. After PS matching, 466 patients, mean age 69±12 years, were analyzed. No significant sex-based differences were observed in 3-year outcomes, including all-cause mortality (HR 1.09; 95% CI, 0.76–1.57), ischemic stroke (HR 0.93; 95% CI, 0.58–1.49), acute myocardial infarction (HR 1.02; 95% CI, 0.73–1.44), new-onset atrial fibrillation (HR 0.87; 95% CI, 0.61–1.23), and incident ESRD (HR 1.33; 95% CI, 0.60–2.93). Similarly, no significant difference was observed in HF readmissions at 6 months (HR 1.09; 95% CI, 0.94–1.25). Conclusion: Our study did not reveal any significant sex-related differences in clinical outcomes among HF patients with CA on SGLT2i. These findings support the need for equitable prescribing practices in this high-risk population.
Bashir, Zubair
(
University of Texas Medical Branch
, Galveston , Texas , United States )
Saxena, Ritika
(
University of Texas Medical Branch
, Galveston , Texas , United States )
Yang, Michelle
(
University of Texas Medical Branch
, Galveston , Texas , United States )
Khalife, Wissam
(
University of Texas Medical Branch
, Galveston , Texas , United States )
Jneid, Hani
(
University of Texas Medical Branch
, Galveston , Texas , United States )
Chatila, Khaled
(
University of Texas Medical Branch
, Galveston , Texas , United States )
Albaeni, Aiham
(
University of Texas Medical Branch
, Galveston , Texas , United States )
Author Disclosures:
Zubair Bashir:DO NOT have relevant financial relationships
| Ritika Saxena:No Answer
| Michelle Yang:No Answer
| Wissam Khalife:DO NOT have relevant financial relationships
| Hani Jneid:DO NOT have relevant financial relationships
| Khaled Chatila:No Answer
| Aiham Albaeni:DO NOT have relevant financial relationships