Phenotypic Sex-Based Differences in Left Ventricular Geometry in Chronic Aortic Regurgitation
Abstract Body (Do not enter title and authors here): Background: Chronic Aortic Regurgitation (AR), a prevalent form of valvular heart disease, is associated with significant mortality and morbidity if left untreated. Emerging studies demonstrate significant sex-specific differences in AR presentation and clinical outcomes, yet current management guidelines do not account for these sex differences. Additionally, females with AR tend to exhibit increased symptoms despite reduced ventricular volume and preserved function.
Research Question: How do left ventricular structure and geometry differ between sexes across varying severities of AR?
Methods: A single-center, retrospective cohort study was conducted and included patients with an aortic regurgitant fraction >20% by cardiac magnetic resonance (CMR) or ≥ moderate AR by echocardiography. AR severity was quantified using regurgitant fraction (ARFrac) thresholds, quantified by CMR (Mild: ARFrac < 20, Moderate: 20 ≤ ARFrac ≤ 33, Severe: ARFrac > 33). Cardiac geometry measured by CMR was determined using LV mass index (LVMassi), left ventricular end diastolic diameter indexed (LVEDDi), LV end systolic diameter index (LVESDi), interventricular septal thickness (IVS), posterior wall thickness (PWT), LV length, and derived indices including relative wall thickness (RWT) and sphericity. Volumetric measures included LVEDVi, LVESVi, and LVEF. Comparisons were stratified by sex, and significance was assessed using Wilcoxon rank-sum tests.
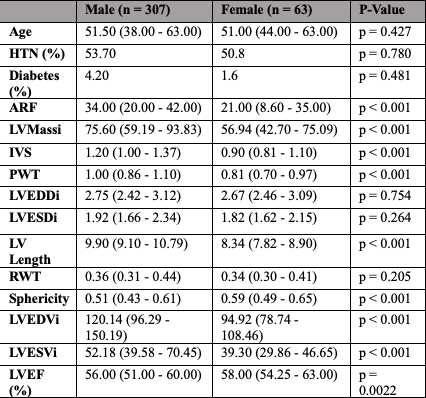
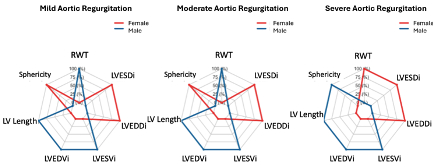
Results: We evaluated 370 patients with AR, 63 female (17%), median age of 51 years. See Table 1 for the comparisons of age, hypertension, diabetes, ARFrac, and LV morphologic features stratified by sex. Radar plots significant sex differences in morphologic features across varying AR severity levels (mild, moderate, and severe). Opposite changes in RWT and sphericity were present in the setting of severe AR, based on sex.
Conclusion: There are evident sex-specific differences in AR LV remodeling. Males exhibit more chamber dilation with increased sphericity and RWT with severe AR, while females maintain smaller, with decreased sphericity and increased RWT in the setting of severe AR. These differences may contribute to disparities in symptom presentation and AR severity. Recognizing sex-based remodeling patterns may inform the future development of more personalized clinical guidelines for AR management, including risk stratification and surgical referral thresholds.
Sonig, Anika
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Deangelo, Lydia
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Grimm, Richard
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Rodriguez, L
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Griffin, Brian
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Popovic, Zoran
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Chen, David
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Nguyen, Christopher
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Kwon, Deborah
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Author Disclosures:
Anika Sonig:DO NOT have relevant financial relationships
| Lydia DeAngelo:No Answer
| Richard Grimm:DO NOT have relevant financial relationships
| L Rodriguez:DO NOT have relevant financial relationships
| Brian Griffin:No Answer
| Zoran Popovic:DO NOT have relevant financial relationships
| David Chen:DO NOT have relevant financial relationships
| Christopher Nguyen:No Answer
| Deborah Kwon:DO have relevant financial relationships
;
Research Funding (PI or named investigator):NIH:Active (exists now)
; Other (please indicate in the box next to the company name):Circle Cardiovascular Imaging - research agreement:Active (exists now)
; Consultant:Pfizer:Active (exists now)