Challenging Case: Acute Type A Aortic Dissection with Multi-Organ Malperfusion
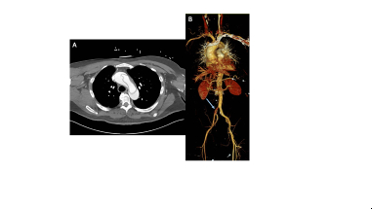
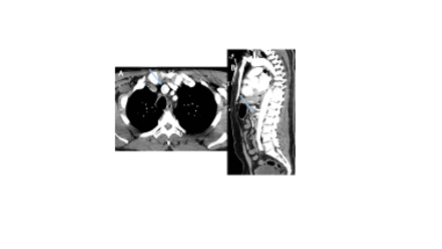
Abstract Body (Do not enter title and authors here): Case Description: A 57-year-old male with hypertension and obesity presented with acute, severe chest pain. He developed a cold, numb right leg with motor deficits. He was hypotensive with a lactate of 7.4. CT imaging revealed an acute Type A aortic dissection (TAAD) with malperfusion involving the right internal carotid, right subclavian, and right coronary arteries, as well as the superior mesenteric artery, and right iliac artery (Fig 1). He was transferred to our tertiary center for emergent surgery.
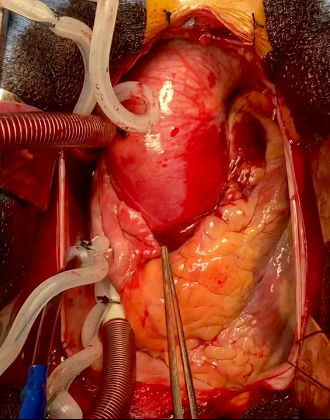
Five hours after presentation, he underwent emergent ascending aortic replacement, deep hypothermic circulatory arrest, and retrograde cerebral perfusion. The dissection flap originated at an anomalous right coronary artery (RCA) arising just above the commissure of the right and left coronary cusps. The proximal aortic wall (adventitia) was extremely thin (Fig 2), and the intimal flap was visibly mobile. Severe aortic insufficiency was addressed with aortic valve repair. Right lower extremity pulse returned with restoration of true lumen flow. Fasciotomy was also performed.
On postoperative day (POD) 1, exploratory laparotomy was performed due to multiple bloody bowel movements, ruling out mesenteric ischemia. He underwent re-exploration and chest closure on POD 2. Postoperative complications included transient delirium, dysphagia, and right diaphragm elevation. He progressed well and was discharged on day 17.
Discussion: Acute TAAD is life-threatening and requires immediate intervention. Organ malperfusion and ischemia can rapidly lead to acidosis, with in-hospital mortality exceeding 85% when more than two organ systems are involved. This patient had malperfusion to five organ systems and a lactate of 7.4, indicating severe metabolic derangement. Although base excess was not measured on presentation, lactate strongly correlates with acidosis, the strongest validated predictor of operative mortality. In this case, a dynamic intimal flap caused intermittent obstruction of branch vessels and coronary flow, worsening ischemia. An anomalous RCA, present in <1% of the population, further complicated the operation. The anomalous origin made surgical manipulation difficult and has been rarely described in the setting of TAAD.
This case was challenging due to multiorgan malperfusion with metabolic acidosis and anatomical complexity. Successful repair and recovery reflect the importance of rapid diagnosis and appropriate management of malperfusion.
Agarwal, Rishab
(
Eastern Virginia Medical School
, Norfolk , Virginia , United States )
Bradshaw, Alleabelle
(
Johns Hopkins University School of Medicine
, Baltimore , Maryland , United States )
Lawton, Jennifer
(
Johns Hopkins University School of Medicine
, Baltimore , Maryland , United States )
Author Disclosures:
Rishab Agarwal:DO NOT have relevant financial relationships
| AlleaBelle Bradshaw:DO NOT have relevant financial relationships
| Jennifer Lawton:DO NOT have relevant financial relationships