Genetic determinants of left ventricular diastolic function
Abstract Body (Do not enter title and authors here): Background Left ventricular (LV) diastolic function relies on active myocardial relaxation and passive cardiac chamber stiffness and is assessed by echocardiography. Abnormal LV diastolic function portends worse outcomes in heart failure (HF), cardiomyopathies, coronary artery disease, and atrial fibrillation. Few studies have evaluated genetic determinants of LV diastolic function.
Methods We meta-analyzed genome-wide association studies (GWAS) for seven quantitative LV diastolic traits measured by echocardiography using data from the Copenhagen Hospital Biobank and previously published GWAS from the EchoGen consortium. Analyzed traits included transmitral flow velocities (E- and A-wave, E/A ratio), E-wave deceleration time, tissue Doppler parameters (average e’, E/e’), left atrial (LA) diameter. We investigated if lead variants were reported in published GWAS for cardiometabolic traits. We next evaluated genetic correlations (rg) between diastolic traits and published GWAS for cardiomyopathies, heart failure subtypes, and MRI-derived diastolic function traits from the UK Biobank.
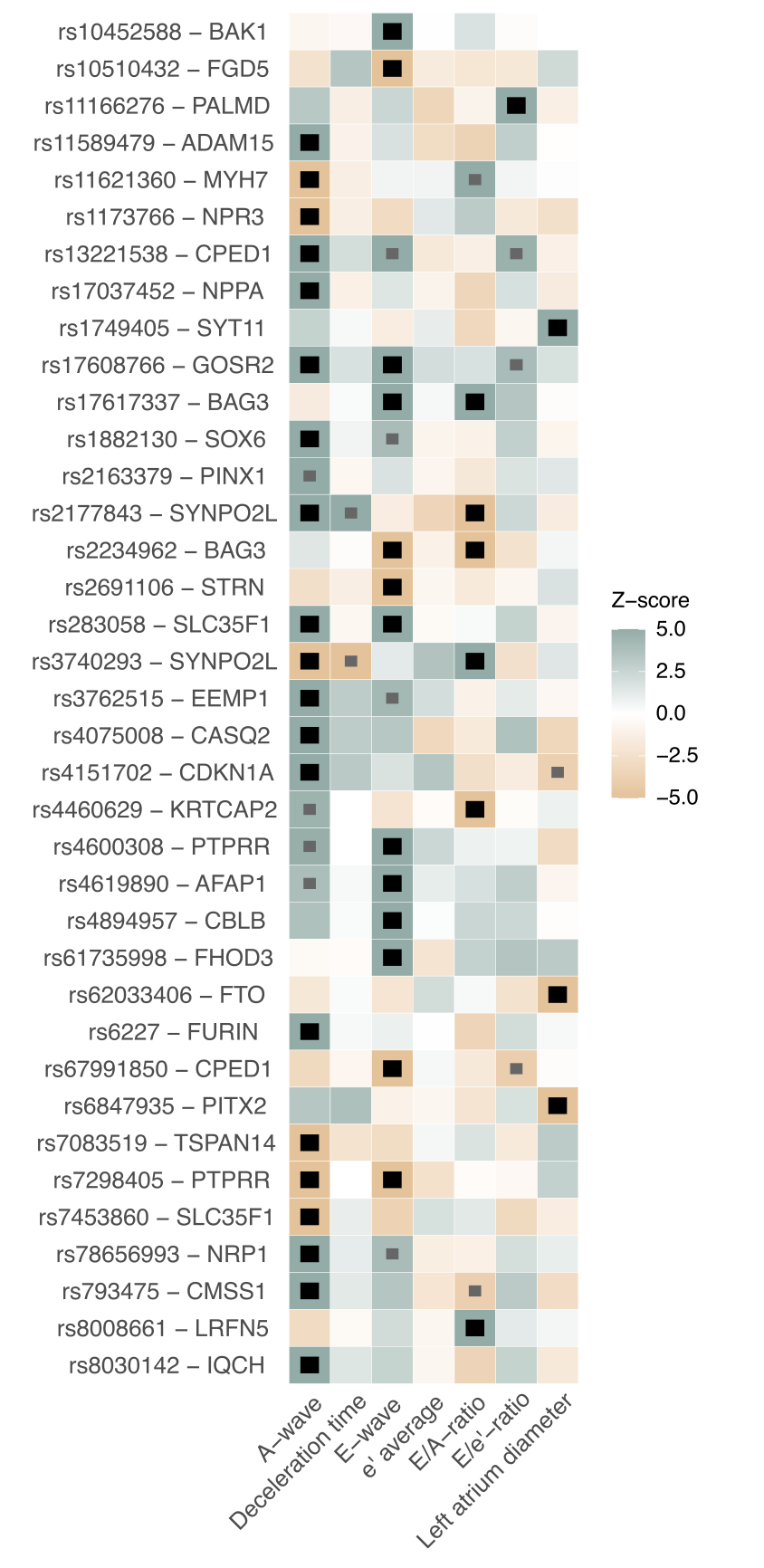
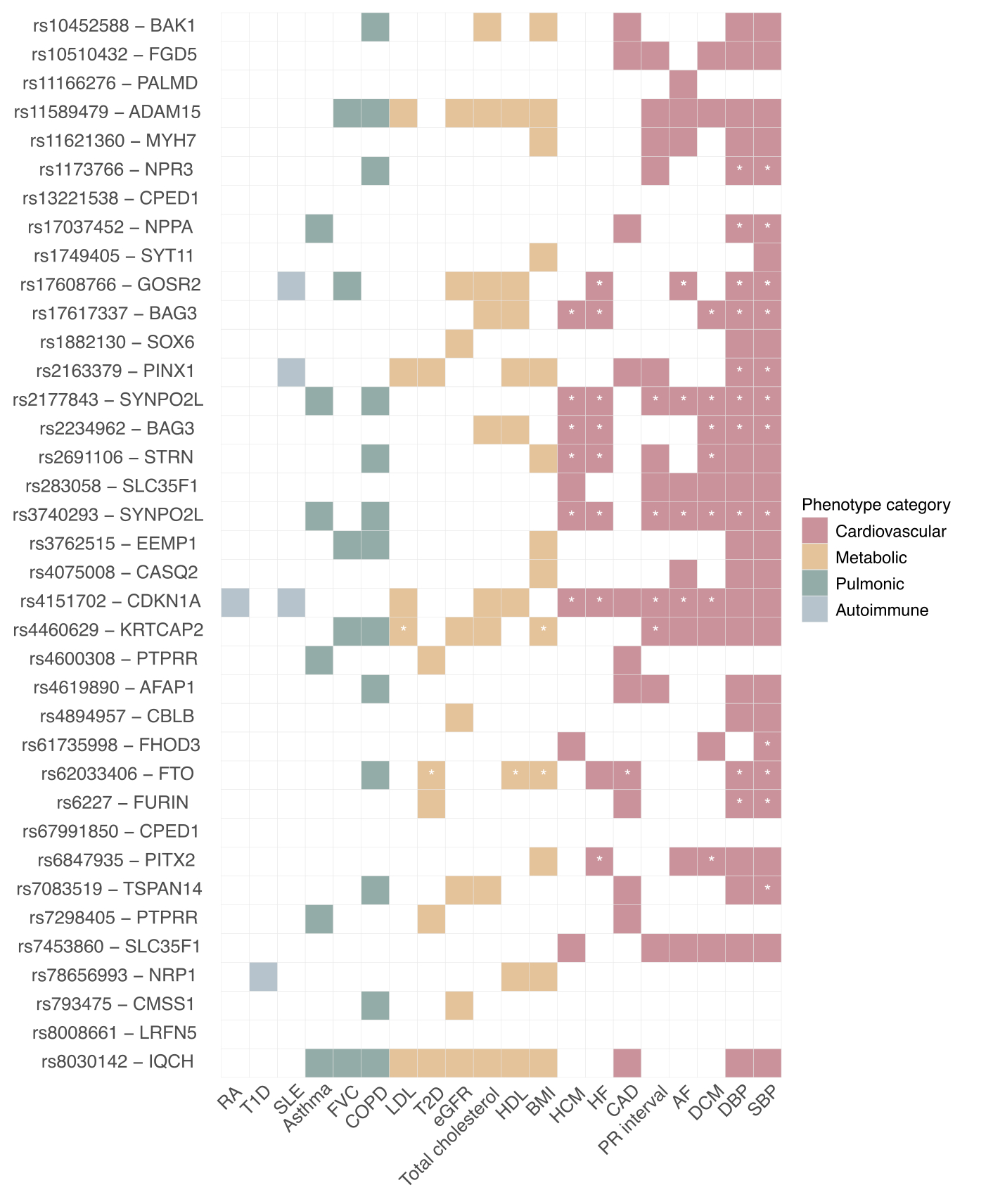
Results Using up to 72,093 individuals for genetic discovery, we identified 37 genome-wide significant independent loci associated with five of seven meta-analyzed traits (Fig.1). Lead variants overlapped with several published cardiometabolic risk loci, most prominently hypertensive traits. Several other were previously implicated in cardiomyopathies (MYH7, BAG3, SYNPO2L, PITX2, FHOD3, STRN, SYNPO2L, CDKN1A; Fig.2), and we also found loci near calcium-handling genes (PLN, CASQ2) and natriuretic peptide signalling genes (ANNP, NPR3). Several LV diastolic traits had strong genetic correlation to cMRI-derived traits (rg range from 0.60 [between E/A-ratio and LV strain] to 0.98 [between average e’ and LA passive emptying fraction]; all P < 1.5×10-5). LA diameter, E- and A-wave had moderate genetic correlation with cardiomyopathies, including HFpEF (rg range 0.31 – 0.54; all P < 0.01).
Conclusion Common genetic variation plays a role in several key components of diastolic function, and are partly underpinned by variants near sarcomere, calcium-handling, and natriuretic signalling genes. Genetic correlation demonstrated that increased early and late diastolic filling as well as increased left atrial diameter positively correlated to HFpEF. Our findings indicate the variety of biological pathways contributing to cardiac diastolic function