An Accessible Image-based Artificial Intelligence-Electrocardiogram Risk Score Enhances Atherosclerotic Cardiovascular Disease Risk Prediction Beyond Traditional Risk Scores
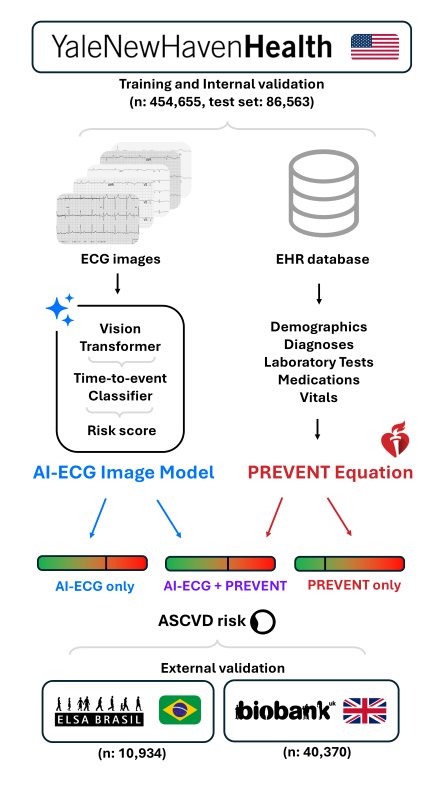
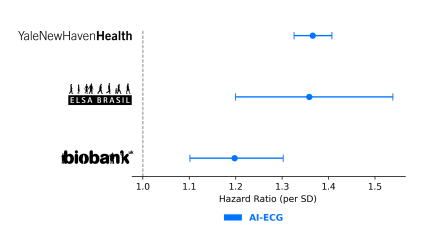
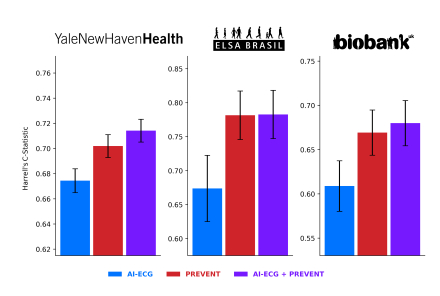
Abstract Body (Do not enter title and authors here): Background: Estimating atherosclerotic cardiovascular disease (ASCVD) risk is crucial in guiding clinical decisions about primary prevention strategies. Well-validated clinical risk scores, such as the Predicting Risk of cardiovascular EVENTs (PREVENT) equations, exist; however, Artificial Intelligence-based inference of electrocardiogram images (AI-ECG) can extract latent prognostic information that may not be captured by traditional risk scores. The additional utility of this widely available and accessible data modality for predicting ASCVD is underexplored. Aims: We sought to (a) develop and validate an AI-ECG risk score for predicting incident ASCVD, (b) assess the incremental prognostic value of AI-ECG over PREVENT. Methods: We identified all adults eligible for PREVENT (30–79 years old without prior CVD) who had undergone a 12-lead ECG in the Yale New Haven Health System (YNNHS) after 2013. ECGs were processed as images with varying layouts by a vision transformer model, whose outputs were used to develop a time-to-event model to predict incident ASCVD. ASCVD was defined by ICD-10 codes (I21, I22, I61, I62, I63) in the EHR. Variables required by PREVENT were extracted, with missing values imputed via MissForest, to calculate corresponding PREVENT scores. Model performance was evaluated using Harrell’s C-statistic, and Cox proportional hazard models were fit to assess additive prognostic information. The model was validated in a held-out YNHHS test set and externally validated in two population-based cohorts: the UK Biobank (UKB) and the Brazilian Longitudinal Study of Adult Health (ELSA). Results: The PREVENT+AI-ECG and AI-ECG models had C-statistics of 0.714 (95% CI, 0.705-0.723) and 0.674 (95% CI, 0.665-0.684) in the YNHHS held-out test set (n=86,563), 0.680 (95% CI, 0.654-0.705) and 0.601 (95% CI, 0.580-0.637) in the UKB (n=42,390), and 0.783 (95% CI, 0.747–0.818) and 0.673 (95% CI, 0.625-0.723) in ELSA (n=10,934) for predicting incident ASCVD. AI-ECG score was an independent risk factor with an adjusted hazard ratio (HR) of 1.37 (95% CI, 1.32-1.40), 1.36 (95% CI, 1.19-1.53), and 1.20 (95% CI, 1.10-1.30) in the UKB and ELSA, respectively. Conclusion: AI-ECG risk scores predict ASCVD risk across diverse multinational cohorts, with evidence for independent risk prediction over the PREVENT equations. This highlights the untapped potential of AI-ECG as a widely deployable strategy to improve the primary prediction and prevention of ASCVD.
Batinica, Bruno
(
Yale University
, New Haven , Connecticut , United States )
Oikonomou, Evangelos
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Dhingra, Lovedeep
(
Yale School Of Medicine
, New Haven , Connecticut , United States )
Pedroso, Aline
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Aminorroaya, Arya
(
Yale University
, New Haven , Connecticut , United States )
Biswas, Dhruva
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Khera, Rohan
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Author Disclosures:
Bruno Batinica:DO NOT have relevant financial relationships
| Evangelos Oikonomou:DO have relevant financial relationships
;
Consultant:Caristo Diagnostics, Ltd:Past (completed)
; Consultant:Ensight-AI, Inc:Active (exists now)
; Ownership Interest:Evidence2Health, LLC:Active (exists now)
| Lovedeep Dhingra:DO NOT have relevant financial relationships
| Aline Pedroso:DO NOT have relevant financial relationships
| Arya Aminorroaya:DO NOT have relevant financial relationships
| Dhruva Biswas:DO NOT have relevant financial relationships
| Rohan Khera:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Bristol-Myers Squibb:Active (exists now)
; Research Funding (PI or named investigator):NovoNordisk:Active (exists now)
; Research Funding (PI or named investigator):BridgeBio:Active (exists now)