Cholesterol Management in US Individuals with ASCVD within the Family Heart Database® during 2022/23: Current State of Care and Opportunities for Improvement
Abstract Body (Do not enter title and authors here):
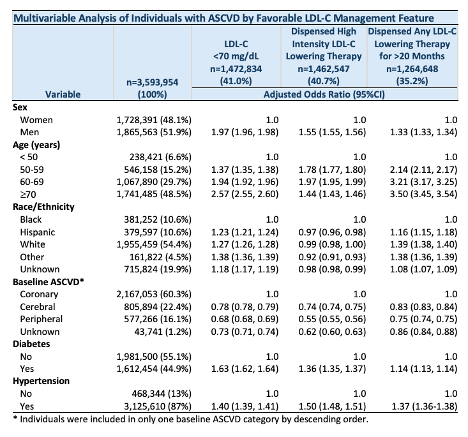
Background: Individuals with atherosclerotic cardiovascular disease (ASCVD) have increased risk of recurrent events and need optimized low density lipoprotein-cholesterol (LDL-C) lowering therapy, yet the factors contributing to LDL-C management, including clinician prescribing patterns, are not well understood. Objective: To characterize the current state of LDL-C management in US individuals with ASCVD and prescribing patterns of clinicians providing care. Methods: A cohort study of the national Family Heart Database during 2022-23 was conducted in individuals with ASCVD and ≥1 medication claim in both years and an LDL-C measure. Clinicians writing ≥5 LDL-C lowering prescriptions were included. The lowest achieved LDL-C level (<55 mg/dL; 55-69 mg/dL; ≥70 mg/dL); highest intensity LDL-C lowering therapy prescribed (high intensity; low/moderate intensity; none); and duration of dispensed LDL-C lowering therapy (>20 of 24 months; 13 to 20 months; >0 to <13 months; none) were characterized. Corresponding percent of clinicians prescribing statin monotherapy and non-statin LDL-C therapies was assessed. Results: The database included adults (n=3,593,954) with ASCVD, mean age 67 years, 48% women, 11% Black individuals, and 7% aged <50 years. Of these, 41% had an LDL-C <70 mg/dL, 41% received high intensity LDL-C lowering therapy, and 35% were dispensed LDL-C lowering therapy for >20 of 24 months; only 13% were found to have LDL-C management across all three of these components. According to multivariable logistic regression models, women, Black individuals, those <50 years old, and those with peripheral arterial and cerebrovascular disease were less well managed (see table). Of 247,318 clinicians, 50% prescribed only statin monotherapy, including 8% who prescribed only low/moderate intensity statins. Only 7308 clinicians (3%) were responsible for prescribing half (50%) of all non-statins; within this group of predominantly cardiologists, the ratio of statin to non-statin prescriptions was 3:1. Conclusions In this cohort of 3.6 million US individuals with ASCVD there was a substantial gap between guideline recommended LDL-C management and clinical care. Several modifiable factors contributed to this gap including low use of non-statin LDL-C therapies in this high risk population.
Macdougall, Diane
(
Family Heart Foundation
, Fernandina Beach , Florida , United States )
Ferdinand, Keith
(
Tulane SOM
, New Orleans , Louisiana , United States )
Baum, Seth
(
Flourish Research
, Boca Raton , Florida , United States )
Sperling, Laurence
(
Family Heart Foundation
, Fernandina Beach , Florida , United States )
Hartsuff, Bonnie
(
BIA Clinical
, Chelsea , Michigan , United States )
Wilemon, Katherine
(
Family Heart Foundation
, Fernandina Beach , Florida , United States )
Nissen, Steven
(
CLEVELAND CLINIC
, Cleveland , Ohio , United States )
Author Disclosures:
Diane MacDougall:DO NOT have relevant financial relationships
| Keith Ferdinand:DO have relevant financial relationships
;
Consultant:Amgen:Active (exists now)
; Consultant:Lilly:Active (exists now)
; Consultant:Boehringer Ingelheim:Active (exists now)
; Consultant:Medtronics:Active (exists now)
; Consultant:Novartis:Active (exists now)
| Seth Baum:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):Altimmune - Consultant/Scientific Advisory Board:Active (exists now)
; Other (please indicate in the box next to the company name):Regeneron - Consultant/Scientific Advisory Board/Speaker:Active (exists now)
; Other (please indicate in the box next to the company name):Novartis - Scientific Advisory Board/Consultant:Active (exists now)
; Consultant:Merck:Active (exists now)
; Other (please indicate in the box next to the company name):Madrigal - Consultant/Scientific Advisory Board:Active (exists now)
; Other (please indicate in the box next to the company name):Ionis - Consultant/Scientific Advisory Board/Speaker:Active (exists now)
; Other (please indicate in the box next to the company name):Esperion - Scientific Advisory Board/Speaker:Active (exists now)
; Other (please indicate in the box next to the company name):Eli Lilly - Scientific Advisory Board/Speaker/Consultant:Active (exists now)
; Other (please indicate in the box next to the company name):Boehringer Ingelheim - :Active (exists now)
; Advisor:Beren Therapeutics - Scientific Advisory Board/Speaker:Active (exists now)
; Other (please indicate in the box next to the company name):Amgen - Consultant/Scientific Advisory Board:Active (exists now)
| Laurence Sperling:DO NOT have relevant financial relationships
| Bonnie Hartsuff:No Answer
| Katherine Wilemon:DO NOT have relevant financial relationships
| Steven Nissen:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Esperion Therapeutics:Active (exists now)
; Research Funding (PI or named investigator):CRSPR Therapeutics:Active (exists now)
; Research Funding (PI or named investigator):Bristol Myers Squibb:Active (exists now)
; Research Funding (PI or named investigator):Kardigan:Active (exists now)
; Research Funding (PI or named investigator):Arrowhead:Active (exists now)
; Research Funding (PI or named investigator):Astra Zeneca:Active (exists now)
; Research Funding (PI or named investigator):New Amsterdam:Active (exists now)
; Research Funding (PI or named investigator):Eli Lilly:Active (exists now)
; Research Funding (PI or named investigator):Novartis:Active (exists now)
; Research Funding (PI or named investigator):Mineralys:Active (exists now)