In-Hospital, 1-Year and 5-Year Clinical Outcomes of Patients With Severe Aortic Stenosis Treated With Transcatheter Aortic Valve Replacement and Sodium-Glucose Cotransporter 2 Inhibitors
Abstract Body (Do not enter title and authors here): Background: Recent studies have demonstrated that sodium-glucose cotransporter 2 inhibitors (SGLT2i) may reduce procedure-related acute kidney injury (AKI), heart failure readmission and late mortality in patients undergoing transcatheter aortic valve replacement (TAVR).
Hypothesis: We sought to investigate the frequency of use and clinical impact on in-hospital and late TAVR outcomes of SGLT2i in a real-world setting in a high volume TAVR center.
Methods: From a total cohort of 3,333 TAVR procedures performed since 2015, we compared in-hospital, 1-year and 5-year clinical outcomes in 241 patients treated with SGLT2i versus 3,092 without SGLT2i use. Patients received SGLT2i (empagliflozin n=181, dapagliflozin propanediol n=54, or canagliflozin n=6) prior to and following TAVR for treatment of heart failure with diabetes, renal insufficiency and/or left ventricular systolic dysfunction. Dialysis patients and valve-in-valve TAVR procedures were excluded. Propensity-matching was used to adjust for co-variates. AKI was defined by VARC-2 criteria.
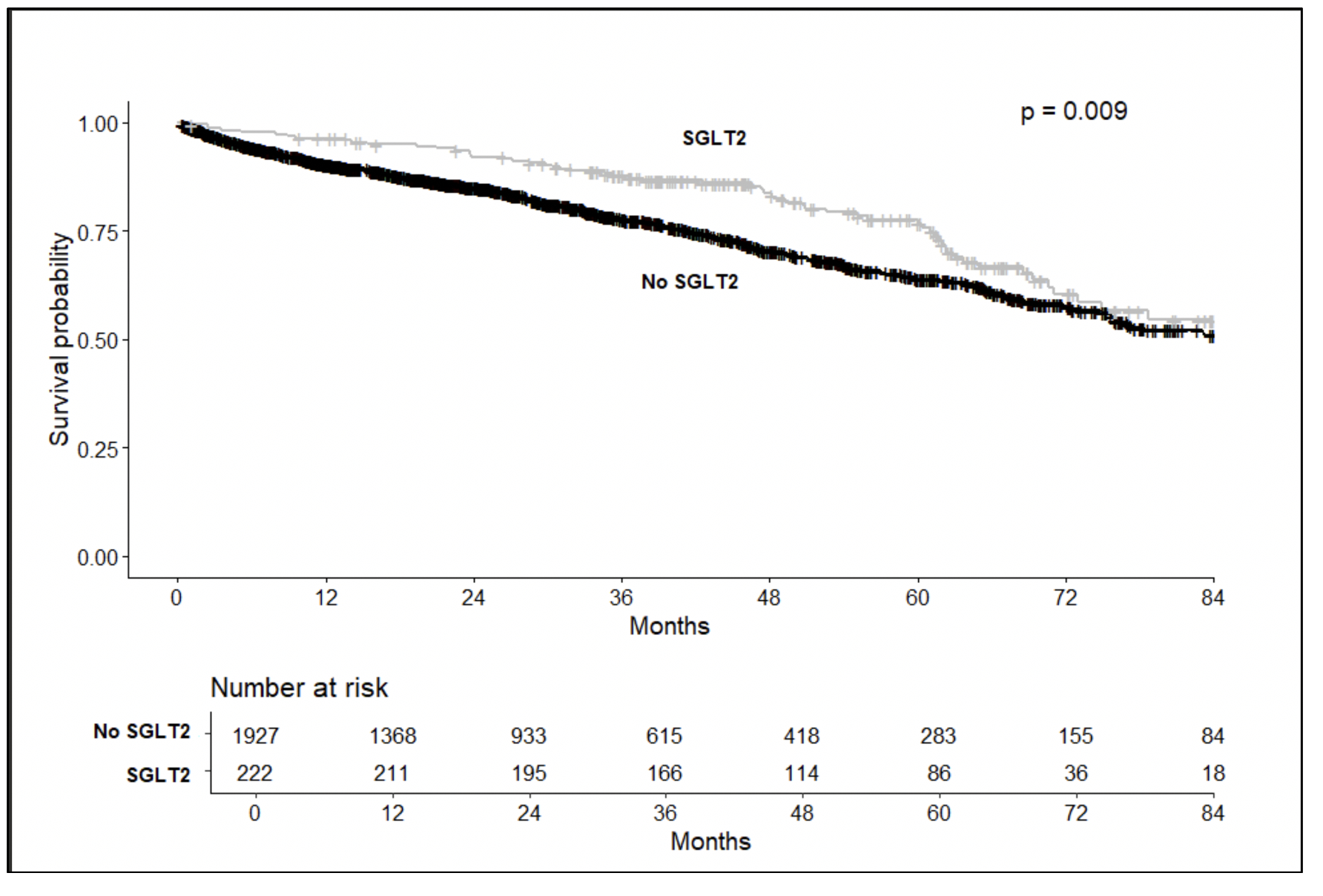
Results: Propensity-matched SGLT2i (n=225) and No SGLT2i (n=1,949) cohorts did not differ with respect to baseline characteristics including age (80.0±6.6 vs. 80.9±8.5 years, p=0.061), sex, creatinine, hemoglobin, NYHA class, pre-TAVR echo and cardiac catheterization findings, and STS score (8.9±7.2% vs. 8.0±6.5%, p=0.063). Both groups had similar use of general/conscious sedation anesthesia, femoral/carotid access, balloon-expandable/self-expanding valve type, fluoroscopy time and contrast load (80.0±42.2 vs 84.0±40.3 ml, p=0.248). SGLT2i versus No SGLT2i patients had similar in-hospital mortality (0.0 vs 0.4%, p=0.0338), ischemic strokes (0.9 vs 1.3%, p=0.575), major vascular complications (2.2 vs 2.5%, p=0.790), and composite bleeding (2.2 vs 2.9%, p=0.576), although SGLT2i patients had a lower incidence of AKI (2.2 vs 6.0%, p=0.020). At 1-year, the SGLT2i group had lower all-cause mortality (3.2 vs 6.6%, p=0.046) but similar hospital readmission rates (19.1 vs 21.7%, p=0.379) and quality of life KCCQ12 scores (81.7±19.0 vs 81.7±19.1, p=0.071). At a mean follow-up of 65.9 (64.2-67.5) months, Kaplan-Meier survival analysis demonstrated lower all-cause mortality in the SGLT2i cohort (p=0.009) (figure).
Conclusion: In this single center study, SGLT2i use was infrequent in patients undergoing TAVR, and was associated with decreased procedural AKI as well as decreased all-cause mortality at 1 and 5-year follow-up.
Thakurathi, Priyesh
(
Hartford Hospital
, Hartford , Connecticut , United States )
Jaiswal, Abhishek
(
Hartford Hospital
, Hartford , Connecticut , United States )
Mather, Jeff
(
Hartford Hospital
, Hartford , Connecticut , United States )
Hagberg, Robert
(
Hartford Hospital
, Hartford , Connecticut , United States )
Haider, Jawad
(
Hartford Hospital
, Hartford , Connecticut , United States )
Hashim, Sabet
(
Hartford Hospital
, Hartford , Connecticut , United States )
Mckay, Raymond
(
Hartford Hospital
, Hartford , Connecticut , United States )
Author Disclosures:
Priyesh Thakurathi:DO NOT have relevant financial relationships
| Abhishek Jaiswal:No Answer
| Jeff Mather:DO NOT have relevant financial relationships
| Robert Hagberg:DO NOT have relevant financial relationships
| Jawad Haider:No Answer
| Sabet Hashim:DO NOT have relevant financial relationships
| Raymond McKay:DO NOT have relevant financial relationships