Overall, Race and Regional trends in Ischemic heart disease mortality among adults with Chronic Kidney Disease: Insights from CDC WONDER (1999–2020)
Abstract Body (Do not enter title and authors here): Background Chronic Kidney Disease (CKD) and Ischemic Heart Disease (IHD)-related mortality is a significant burden among US adults. This study investigates trends in CKD and IHD-related mortality in adults aged 25 and older focusing on overall, geographic, and racial/ethnic disparities from 1999 to 2020.
Methods A retrospective analysis was conducted using death certificate data from the CDC WONDER database from 1999 to 2020. Age-adjusted mortality rates (AAMRs), annual percent change (APC), and average annual percentage change (AAPC) were calculated per 100,000 persons, stratified by year, sex, race/ethnicity, and geographical region.
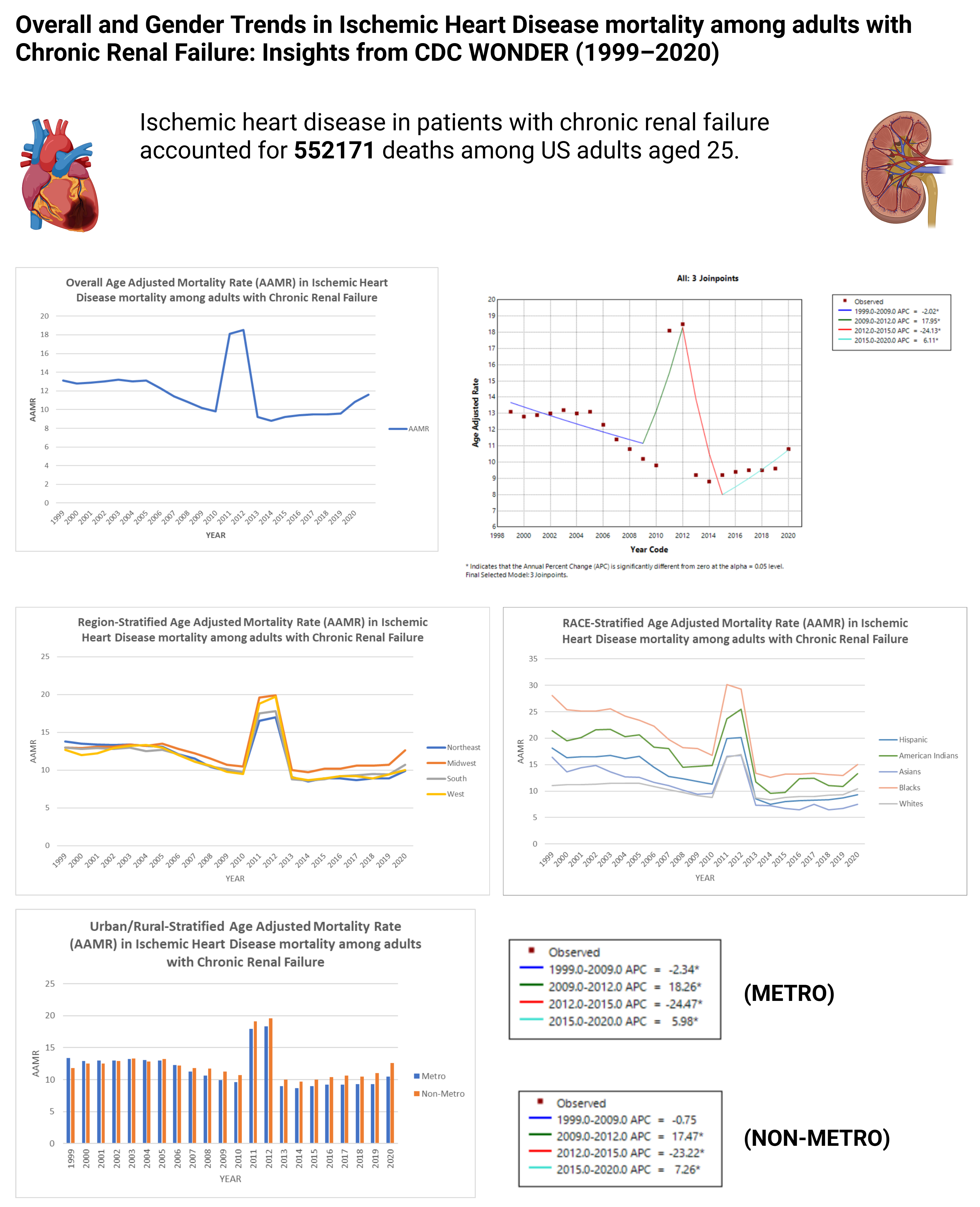
Results CKD and IHD-related mortality accounted for 552171 deaths among US adults aged 25+. Most deaths occurred at a medical facility (45.30%) and the patient’s home (19.90%). The overall AAMR decreased from 13.1 in 1999 to 10.8 in 2020, with an AAPC of -1.1378 (95 % CI: -4.1816 to 2.0028, p = 0.473276). It is worth noting from 2015 to 2020 the APC has been 6.1116 (95 % CI: 2.1479 to 10.2291, p = 0.005627) suggesting an acute rise. Racial/ethnic disparities showed the highest AAMRs in Blacks (19), followed by American Indians (15.7), Hispanics (12), Whites (10.6), and Asians (9.9). Over the years, racial stratification showed a decrease in mortality among all races. The most significant decrease was in Asians (AAPC: -4.0767, p = 0.000034) and Hispanics (AAPC: -3.8230, p = 0.000122). Geographically, AAMRs ranged from 5.6 in Nevada to 18.3 in West Virginia, with the highest mortality observed in the Midwest (AAMR: 12.4) followed by the West (AAMR: 11.4). Over the years, the mortality has been decreasing in all the regions with the most significant decline being in the Northeastern (AAPC of -2.3167, p = 0.000741) followed by the Western states (AAPC of -1.8062, p = 0.046572). Nonmetropolitan areas exhibited higher AAMRs (12.2) than metropolitan areas (11.4). Overall trends (1999 to 2020) show a decline in mortality for both metro and non-metro however from 2015 to 2020 the mortality has increased in both areas with a sharper increase in the non-metropolitan areas (APC: 7.2592, p = 0.001435) than in the metropolitan areas (APC: 5.9817, p = 0.008059).
Conclusion We believe better cardiorenal interventions are required to combat this acute rise of the IHD burden in CKD patients with a special focus on the Black and American Indian populations, the Midwest, and non-metropolitan areas.
Abid, Hassaan
(
Indiana University School of Medicine
, Muncie , Indiana , United States )
Patel, Nandan
(
AIIMS, Jodhpur
, Vadodara , India )
Sighaka Sighaka, Damien
(
Indiana University School of Medicine
, Muncie , Indiana , United States )
Saleh, Akrum
(
Indiana University School of Medicine
, Muncie , Indiana , United States )
Jain, Hritvik
(
AIIMS, Jodhpur
, Vadodara , India )
Author Disclosures:
Hassaan Abid:DO NOT have relevant financial relationships
| Nandan Patel:DO NOT have relevant financial relationships
| Damien Sighaka Sighaka:DO NOT have relevant financial relationships
| Akrum Saleh:DO NOT have relevant financial relationships
| Hritvik Jain:DO NOT have relevant financial relationships
Kane Jamie, Collins Jeremy, Lee Timmy, Misra Sanjay, Singh Prabh, Kilari Sreenivasulu, Baranwal Gaurav, Naskar Atanu, Montonye Dan, Lutgens Esther, Wang Ying, Negm Ahmed