Regional Differences in Outcomes in Adults after Percutaneous Coronary Intervention (PCI) for Stable Ischemic Heart Disease
Abstract Body (Do not enter title and authors here): Background: Previous studies on Percutaneous Coronary Intervention (PCI) for Acute Coronary Syndrome (ACS) have found a disparate distribution of healthcare resources across U.S. regions, contributing to regional differences in cardiovascular outcomes. Whether regional variation in clinical outcomes exist among patients with Chronic Coronary Disease (CCD) who undergo PCI remains unknown.
Research question: Does regional variation affect clinical outcomes in patients with chronic coronary disease undergoing percutaneous coronary intervention in the United States?
Methods: We included patients undergoing PCI for CCD between January 2016 and June 2022 using the Vizient® Clinical Database. We evaluated major adverse cardiovascular events (MACE) — encompassing in-hospital all-cause mortality, myocardial infarction (MI), or repeat coronary revascularization by PCI or CABG — across hospitals in the South, Northeast, Midwest, and West within one year of the index PCI. We also assessed secondary outcomes, including individual components of the composite, major bleeding, and cardiovascular-related hospitalizations. We adjusted for demographics, comorbidities, hospital characteristics, encounter information, and procedural information.
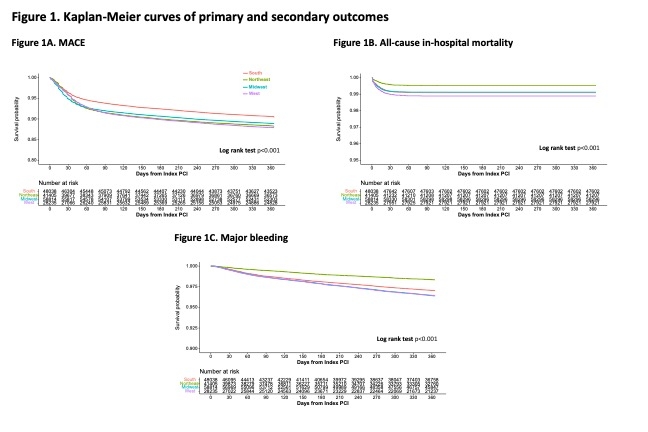
Results: A total of 176,492 patients were included across 176 hospitals, with 22% of patients from hospitals in the South, 23.46% Northeast, 33.32% Midwest, and 16% from the West. When compared with hospitals in the South as the reference, all other regions had higher risk of MACE and repeat PCI (Figure 1). After adjusting for covariates, patients cared for in Midwest hospitals had a higher risk of MACE (relative risk [RR] 1.24, 95% Confidence Interval [CI] 1.19-1.30), all-cause in-hospital mortality (RR 1.25, 95% CI 1.09-1.43), MI (RR 1.37, 95% CI 1.24-1.51), major bleeding(RR 1.33, 95% CI 1.23-1.44), cardiovascular-related hospitalizations (RR 1.04, 95% CI 1.01-1.08), renal replacement therapy (RR 1.41, 95% CI 1.19-1.66), and repeat PCI (RR 1.21, 95% CI 1.15-1.27). In contrast, patients in the Northeast had the lowest relative risk of mortality (RR 0.69, 95% CI 0.57-0.84) and major bleeding (RR 0.72, 95% CI 0.64-0.81).
Conclusion: Significant regional variation exists in clinical outcomes following PCI in patients with CCD. Understanding driving factors for these disparities represents a target for future quality improvement efforts.
Akman, Zafer
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Park, Dae Yong
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Rossi, Raiza
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Nouri, Armin
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Arya Nezhad, Shefa
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Al Mouslmani, Mohammad
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Chi, Kuan Yu
(
Jacobi Medical Center
, Bronx , New York , United States )
Lapetina Arroyo, Roberto
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Nanna, Michael
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Author Disclosures:
Zafer Akman:DO NOT have relevant financial relationships
| Dae Yong Park:DO NOT have relevant financial relationships
| Raiza Rossi:DO NOT have relevant financial relationships
| Armin Nouri:DO NOT have relevant financial relationships
| Shefa Arya Nezhad:DO NOT have relevant financial relationships
| Mohammad AL Mouslmani:DO NOT have relevant financial relationships
| Kuan Yu Chi:DO NOT have relevant financial relationships
| Roberto Lapetina Arroyo:DO NOT have relevant financial relationships
| Michael Nanna:DO have relevant financial relationships
;
Consultant:HeartFlow, Inc.:Active (exists now)
; Consultant:Merck:Active (exists now)
; Consultant:Novo Nordisk:Active (exists now)