The U-CLEAR Study: Uncovering Hemodynamic and Vascular Contributors to Chronic Refractory Lower Extremity Edema
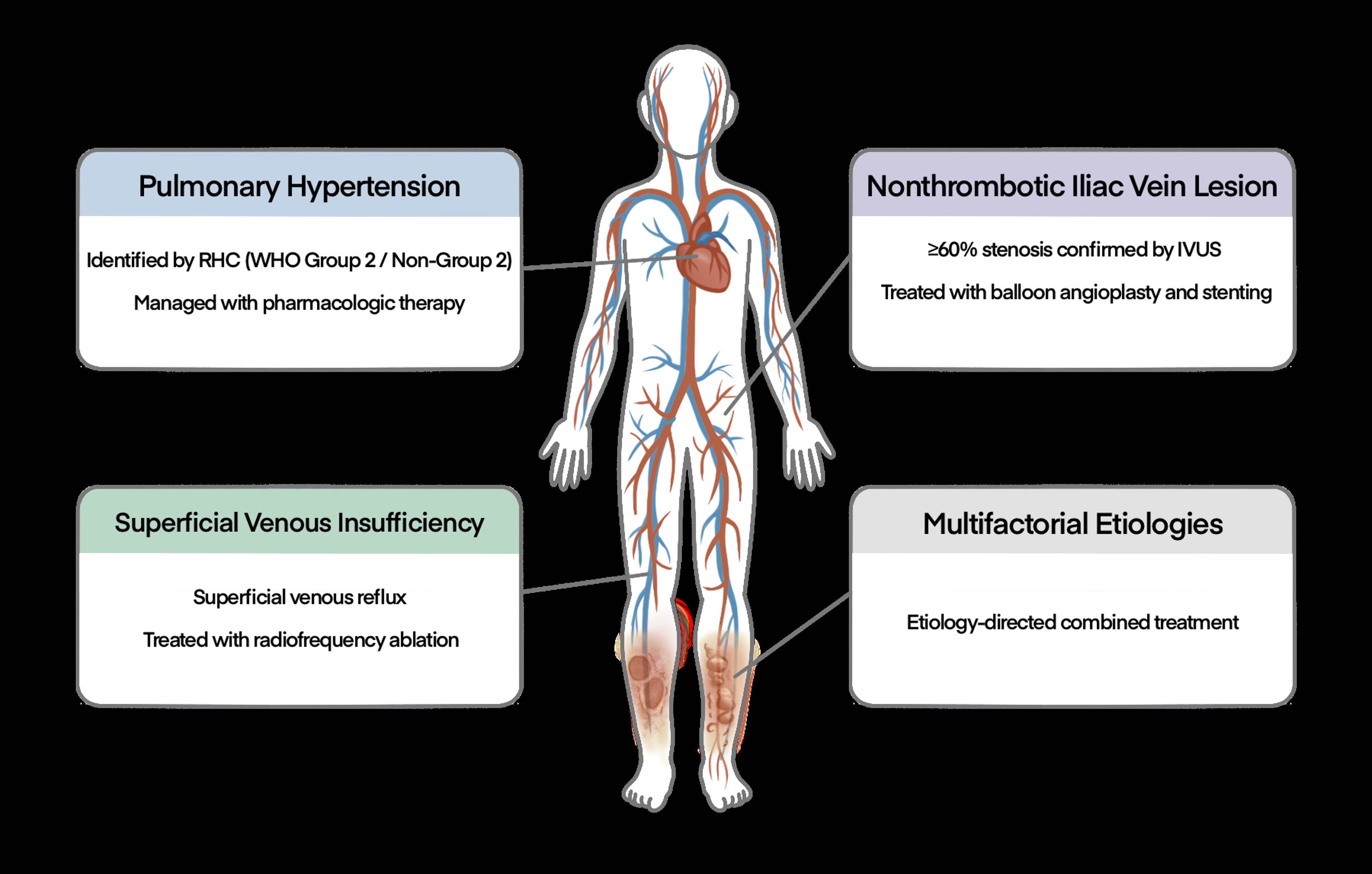
Abstract Body (Do not enter title and authors here): Background Chronic refractory edema in the lower extremities is a disabling condition characterized by persistent swelling and venous stasis skin changes, despite standard conservative therapies. Research Question What are the underlying etiologies of chronic refractory lower extremity edema, and how effective is a structured, integrated diagnostic protocol in improving etiologic classification and guiding targeted management? Study Design and Methods This was a single-center, retrospective analysis of 58 prospectively enrolled patients with chronic, refractory lower extremity edema persisting for ≥1 year, all of whom underwent a standardized diagnostic protocol. Superficial and deep venous insufficiency were assessed using duplex ultrasonography with reflux testing. Central venous anatomy was evaluated with iliocaval ultrasonography to detect potential obstructions in the inferior vena cava or iliac veins. Right heart catheterization was performed to assess for pulmonary hypertension, a possible contributor to chronic venous hypertension in the lower extremities. Iliocaval venography and intravascular ultrasound were employed to confirm or exclude obstructive pathology of the central veins. Right heart catheterization and invasive venous assessments were conducted concurrently. Etiologies were categorized as cardiopulmonary (pulmonary hypertension [PH]), central (non-thrombotic iliac vein lesion [NIVL]), peripheral (superficial venous insufficiency [SVI]), or multifactorial. Results Of the 58 patients, 51.7% had a single identifiable etiology, while 41.4% had multifactorial causes. Non-thrombotic iliac vein lesion (NIVL) was the most common etiology, identified in 55.2% of cases, followed by pulmonary hypertension (PH) in 48.3%, and superficial venous insufficiency (SVI) in 43.1%. Among patients with multifactorial etiologies, NIVL frequently coexisted with either PH or SVI. Unknown etiology, not attributable to any of the specified categories (NIVL, PH, or SVI), was identified in 6.7% of patients. Endovascular intervention for iliocaval obstruction (n = 23) and venous ablation for isolated SVI (n = 10) led to sustained clinical improvement, with no recurrence or procedural complications observed during follow-up. Interpretation This pathophysiology-based diagnostic algorithm enabled accurate etiologic classification and informed individualized treatment strategies for patients with chronic refractory edema and chronic venous skin changes of the lower extremities.
Park, Kyutae
(
UConn Health
, Farmington , Connecticut , United States )
Lee, Juyong
(
UConn Health
, Farmington , Connecticut , United States )
Author Disclosures:
Kyutae Park:DO NOT have relevant financial relationships
| Juyong Lee:DO NOT have relevant financial relationships