Prediction of Aspiration Pneumonia After Cardiac Surgery Using Preoperative Oral Frailty: A Logistic Model
Abstract Body (Do not enter title and authors here): Background: Aspiration pneumonia is a serious complication after cardiac surgery, particularly among older patients. Preoperative oral frailty—decline in oral function including poor hygiene and impaired swallowing—may predispose patients to aspiration. We aimed to develop a risk prediction model for aspiration pneumonia based on oral frailty and other clinical factors in cardiac surgery patients.
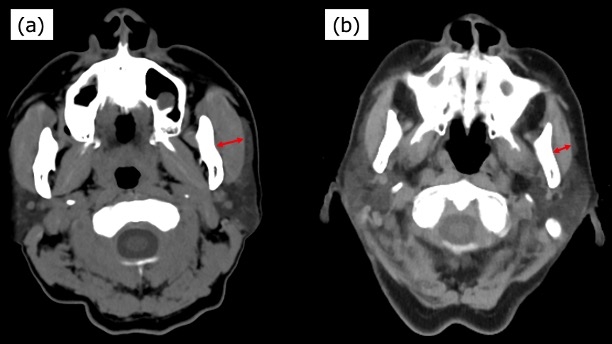
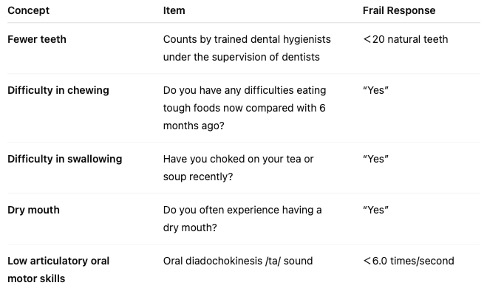
Methods: This retrospective cohort study included 275 consecutive adult patients (median age, 72 years) who underwent elective cardiac surgery between July 2021 and December 2023. Preoperative oral frailty was assessed using the Oral Frailty 5-item Checklist (OF-5; subjective) and masseter muscle thickness on CT (objective; muscle loss defined as ≤25th percentile: males ≤10 mm, females ≤8 mm). Independent predictors of aspiration pneumonia were identified by multivariable logistic regression. Model performance was evaluated using ROC analysis and internally validated using bootstrap resampling to correct for optimism.
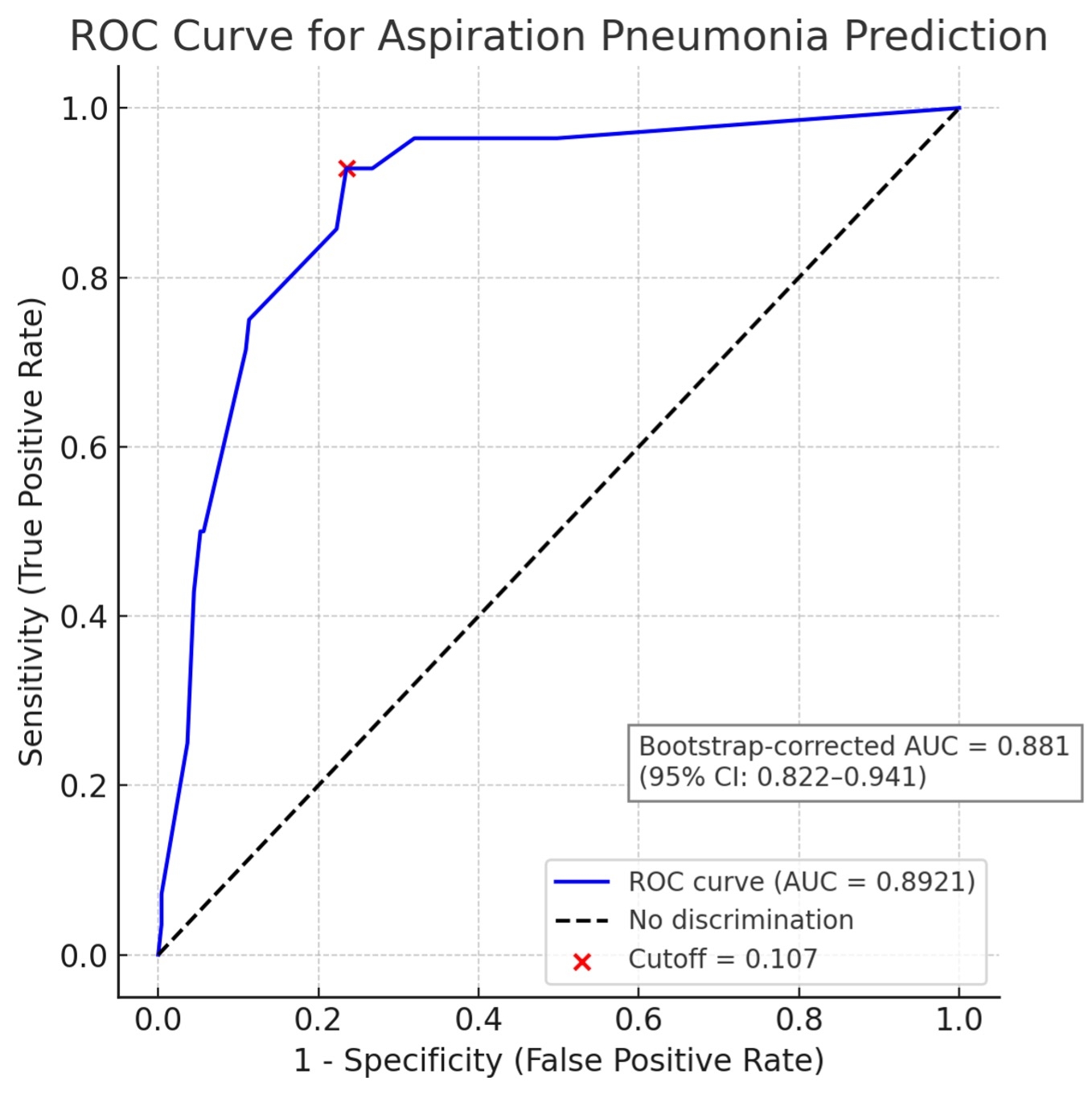
Results: Aspiration pneumonia occurred in 28 patients (10%). Significant predictors included low masseter thickness (OR 11.4, p<0.001), preoperative surgical risk score ≥8% (OR 4.8, p=0.002), COPD (OR 3.9, p=0.023), and OF-5 score ≥2 (OR 2.2, p=0.117). The final logistic regression model was expressed as: logit(p) = –4.4872 + 0.7952×(OF-5≥2) + 2.4326×(Masseter≤25th) + 1.3496×(COPD) + 1.5686×(Risk score≥8%). The logistic model demonstrated excellent discrimination (AUC = 0.892; 95% CI: 0.833–0.951). With a predicted probability cutoff of ≥10.7%, the model achieved 89% sensitivity and 78% specificity. Bootstrap-corrected AUC was 0.881 (95% CI: 0.822–0.941), indicating strong model generalizability. High-risk patients (≥10.7% predicted probability) had significantly worse outcomes than low-risk patients, including aspiration pneumonia (24.8% vs. 1.2%, p<0.001), longer hospital stays (median 20 vs. 14 days, p<0.001), and higher rehabilitation transfer rates (17.1% vs. 4.7%, p<0.001).
Conclusions: Preoperative oral frailty, when incorporated into a logistic regression–based model, accurately predicts aspiration pneumonia following cardiac surgery. Bootstrap validation confirmed the model’s robustness. This tool may support risk stratification and guide preventive strategies to improve perioperative outcomes.
Morimoto, Kenichi
(
Tottori University
, Tottori , Japan )
Kishimoto, Yuichiro
(
Tottori University
, Tottori , Japan )
Onohara, Takeshi
(
Tottori University
, Tottori , Japan )
Horie, Hiromu
(
Tottori University
, Tottori , Japan )
Sasami, Tsuyoshi
(
Tottori University
, Tottori , Japan )
Sumi, Naoki
(
Tottori University
, Tottori , Japan )
Nii, Rikuto
(
Tottori University
, Tottori , Japan )
Kishimoto, Nozomi
(
Tottori University
, Tottori , Japan )
Tokutome, Junpei
(
Tottori University
, Tottori , Japan )
Nakashima, Junya
(
Tottori University
, Tottori , Japan )
Yoshikawa, Yasushi
(
Tottori University
, Tottori , Japan )