Comparison of Linear Ablation Plus Pulmonary Vein Isolation Versus Pulmonary Vein Isolation Alone for Persistent Atrial Fibrillation: Results from the PROMPT-AF Randomized Trial
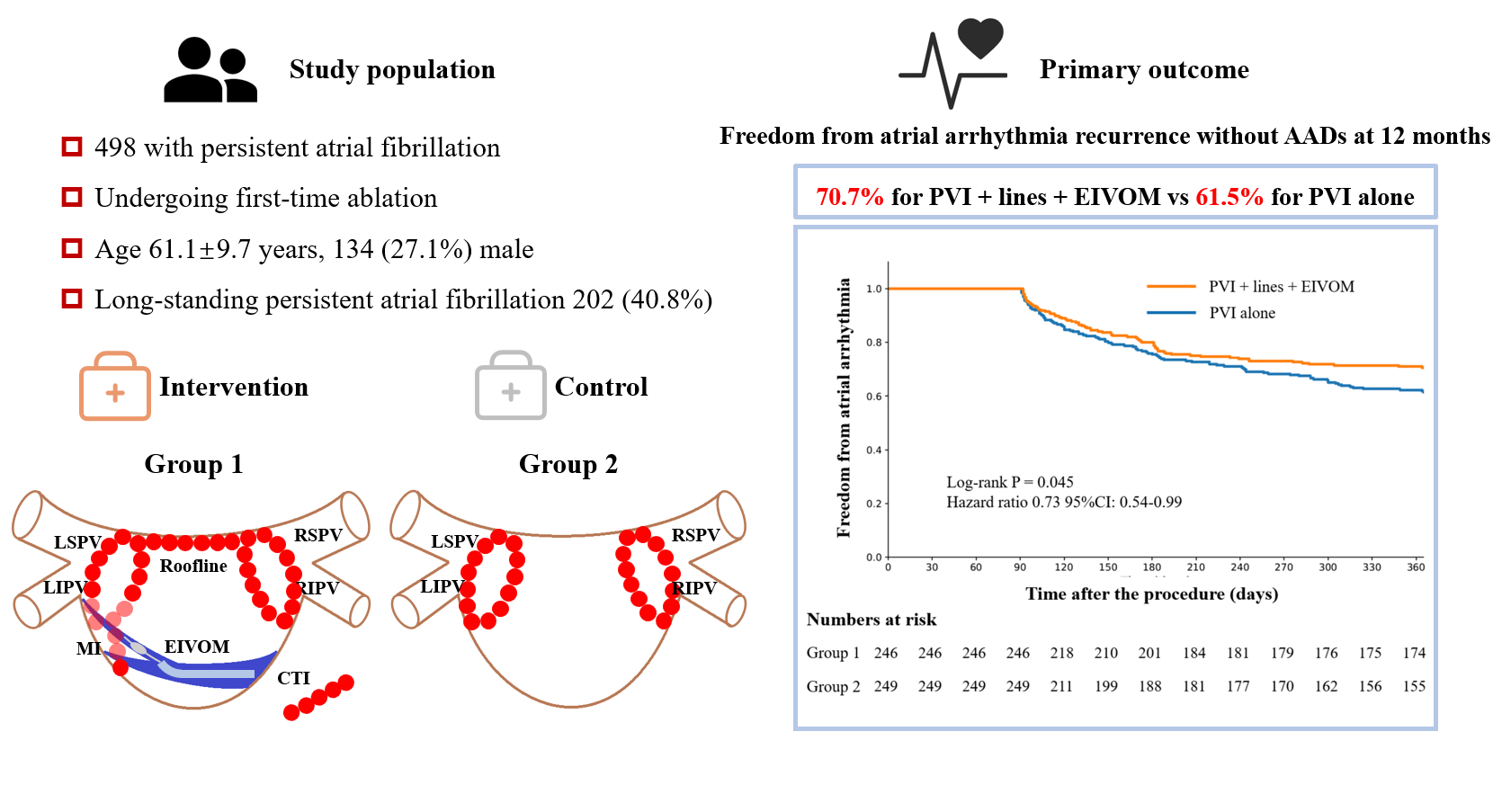
Abstract Body (Do not enter title and authors here): Background: Pulmonary vein isolation (PVI) alone is insufficient for persistent atrial fibrillation (AF) ablation, and the additional benefit of linear ablation beyond PVI has not been confirmed. Vein of Marshall ethanol infusion (EIVOM) facilitates mitral isthmus ablation, optimizing linear ablation approach. Hypothesis and purpose: To determine if the addition of linear ablation combined with EIVOM to PVI significantly outperforms PVI alone in maintaining sinus rhythm. Study design and methods: The PROMPT-AF trial (NCT04497376) is a investigator-initiated, multi-center, open-label, randomized trial. Sample size: 498, randomized in a 1:1 ratio to either intervention or control group. Population studied: Patients with persistent AF over 3 months undergoing first-time AF ablation. Interventions: For intervention (PVI + lines + EIVOM group), EIVOM was performed first, followed by PVI and linear ablation of the left atrial roof, mitral isthmus, and cavo-tricuspid isthmus. For control (PVI alone group), only pulmonary vein isolation was performed. Power Calculation: The sample size provides a power of 0.9, assuming the primary endpoint was achieved in 55% in group 1 and 40% in group 2, respectively, with 10% lost to follow-up. Primary endpoint: Freedom from any documented atrial arrhythmias lasting >30 seconds without anti-arrhythmic drugs (AADs) at12 months post-procedure. Arrhythmia recurrence was monitored using wearable single-lead ECG patches for 24 hours per week, along with any additional symptom-triggered ECGs and Holter monitoring. Arrhythmias detected by the wearable devices were adjudicated by two independent physicians who were blinded to the randomization process. Secondary endpoints: Included atrial arrhythmia recurrence with or without AADs, AF burden, improvement in quality of life, and procedural complications. Outcomes: Among 498 randomized patients, 495(99.4%) were included in the primary analysis. After12 months, 174 patients (70.7%) assigned to PVI + lines + EIVOM and 153 patients (61.5%) assigned to PVI alone remained free from atrial arrhythmias without antiarrhythmic drugs (Hazard ratio 0.73, 95% CI: 0.54 – 0.99, log-rank P = 0.045). (Figure 1). Conclusions: In patients with persistent AF, linear ablation combined with EIVOM in addition to PVI significantly improves freedom from atrial arrhythmias without AADs compared with PVI alone.