Myeloperoxidase Inhibition with Mitiperstat in Heart Failure with Preserved and Mildly Reduced Ejection Fraction: Primary Results from the ENDEAVOR Randomized Clinical Trial
Abstract Body (Do not enter title and authors here): Hypothesis/Purpose: Myeloperoxidase (MPO), an inflammatory mediator released by neutrophils, has been associated with microvascular dysfunction, myocardial fibrosis, and cardiomyocyte dysfunction. We hypothesized that MPO may be a novel treatment target for HFpEF.
Study Design/Methods: Multicenter, randomized, placebo-controlled, double-blind trial of the MPO inhibitor mitiperstat vs. placebo (NCT04986202), conducted from 2021–2024 at 142 sites in 18 countries.
Population Studied: Symptomatic HF (NYHA class II-IV) with LVEF >40%; KCCQ-TSS ≤90 points, 6MWD 30–400 meters; ↑NTproBNP; and (1) structural heart disease, (2) ↑LV filling pressure, (3) significant diastolic dysfunction, or (4) recent HF hospitalization.
Intervention: 48-wk treatment with mitiperstat 2.5 mg, mitiperstat 5.0 mg, or placebo (randomized 1:1:1, stratified by baseline neutrophil count [≤4 vs. >4 K/uL]).
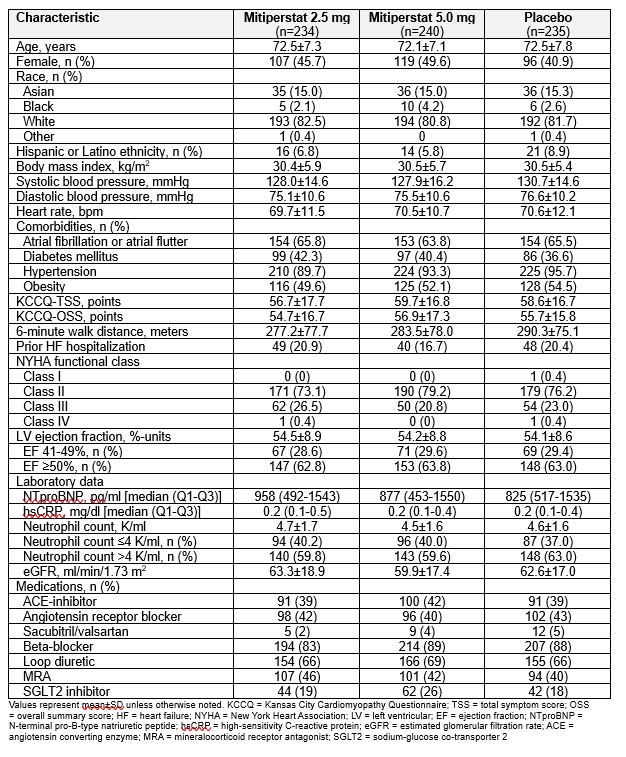
Primary End Points: Change in KCCQ Total Summary Score (KCCQ-TSS) and 6-minute walk distance (6MWD) from baseline to 16 wks. An ANCOVA model was used to estimate treatment effects of mitiperstat vs. placebo.
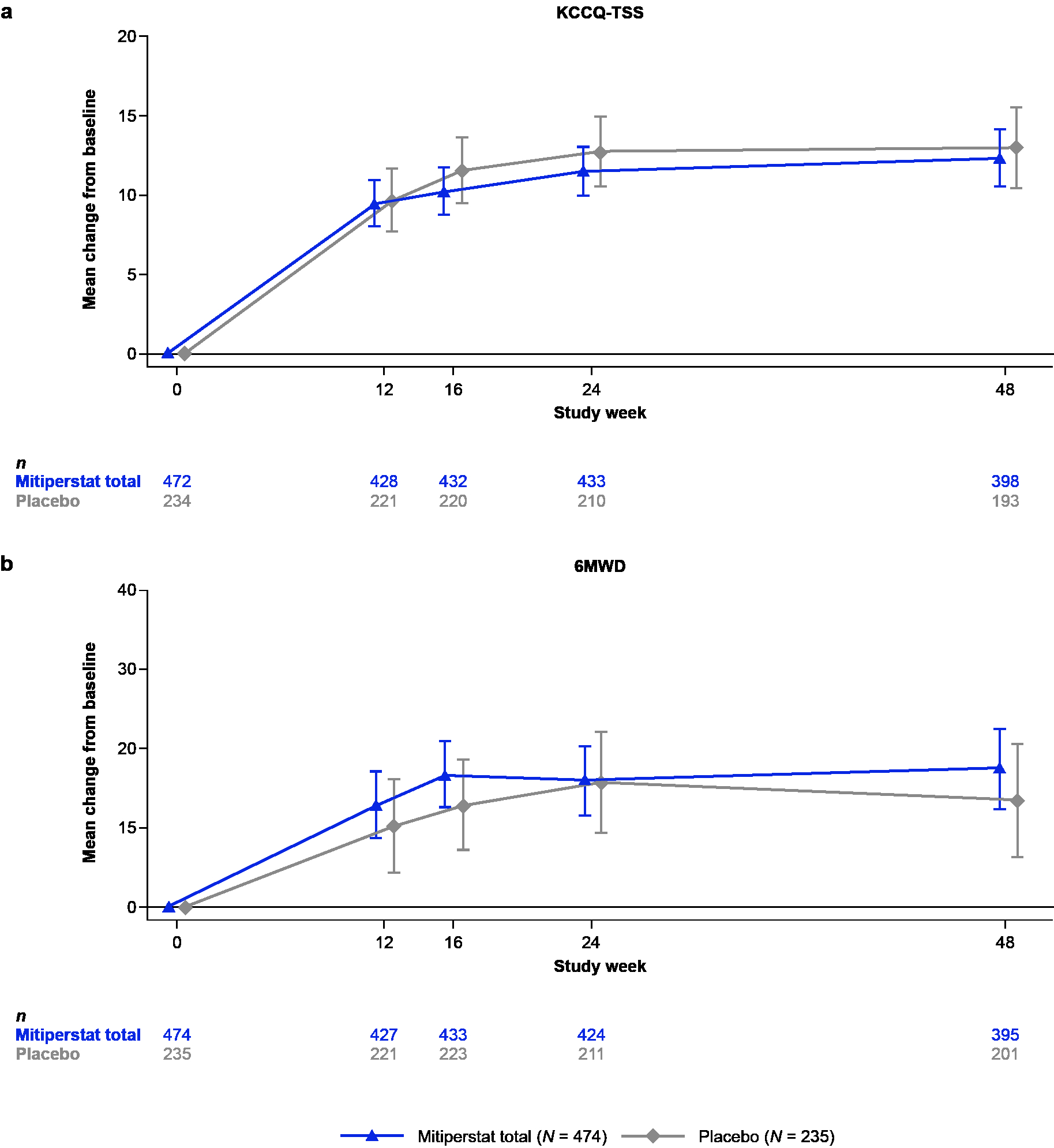
Secondary End Points: Changes from baseline in KCCQ-TSS and 6MWD (24 and 48 wks); biomarkers (NTproBNP, CRP, IL-6; 6, 24, and 48 wks); and echo parameters (LV global longitudinal strain, LVMI, and LAVI; 16 and 24 wks). A composite CV endpoint (HF hospitalization, MI, or death during 48 wks of treatment) was an exploratory endpoint.
Power Calculations: Sample size of 600 (n=200 per arm [n=400 pooled 2.5 and 5.0 mg mitiperstat and n=200 placebo]) provided 85% power at α=0.05 to detect a minimum between-group difference of 6.0 points for △KCCQ-TSS (assumed SD=20 points) and 21 m for △6MWD (assumed SD=70 m).
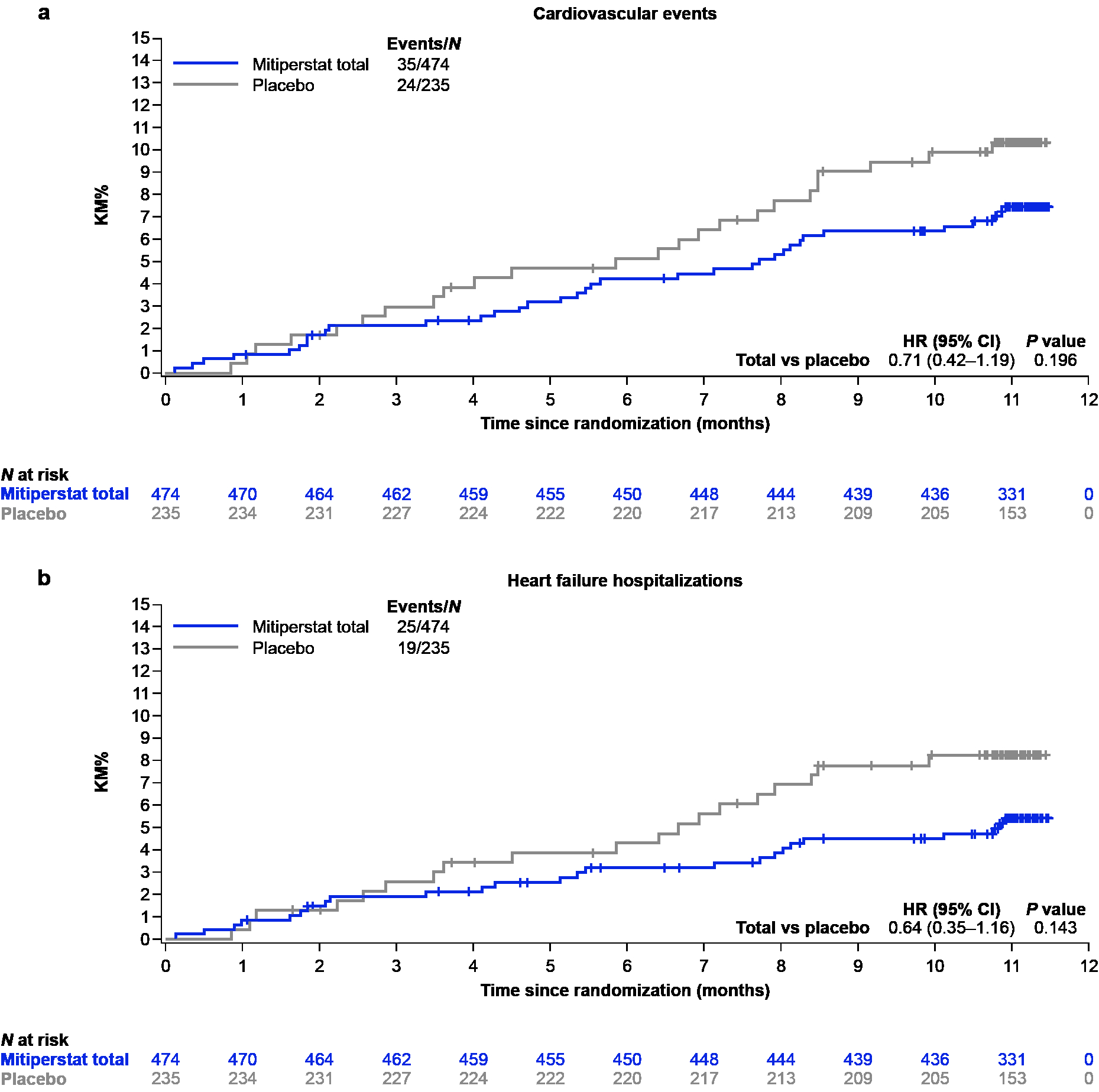
Results: Table 1 displays baseline characteristics. Mitiperstat (2.5 mg + 5.0 mg groups pooled) vs. placebo did not improve KCCQ-TSS or 6MWD (Fig. 1), or any of the secondary endpoints. Results were similar across pre-specified subgroups. Mitiperstat (vs. placebo) resulted in numerically fewer CV events (HR 0.71 [95% CI 0.42, 1.19]; P=0.20) and fewer HF hospitalizations (HR 0.64 [95% CI 0.35, 1.16]; P=0.14) (Fig. 2). AEs and SAEs were similar across groups.
Conclusions: Mitiperstat was safe but did not improve symptoms or exercise function over 16 weeks in HFpEF. The potential beneficial longer-term effect of mitiperstat on reducing HF hospitalization and death requires further investigation.
Lund, Lars
(
Karolinska University Hospital
, Stockholm , Sweden )
Lam, Carolyn
(
National Heart Centre Singapore
, Singapore , Singapore )
Ely Pizzato, Patricia
(
AstraZeneca
, Gothenburg , Sweden )
Michaëlsson, Erik
(
AstraZeneca
, Gothenburg , Sweden )
Mattsson, Andrea
(
AstraZeneca
, Gothenburg , Sweden )
Ericsson, Hans
(
AstraZeneca
, Gothenburg , Sweden )
Baldus, Stephan
(
University Hospital Cologne
, Cologne , Germany )
Shah, Sanjiv
(
Northwestern University
, Chicago , Illinois , United States )