Validation of PAINESD Score to Predict Outcomes of Catheter ablation of Structural Ventricular Tachycardia
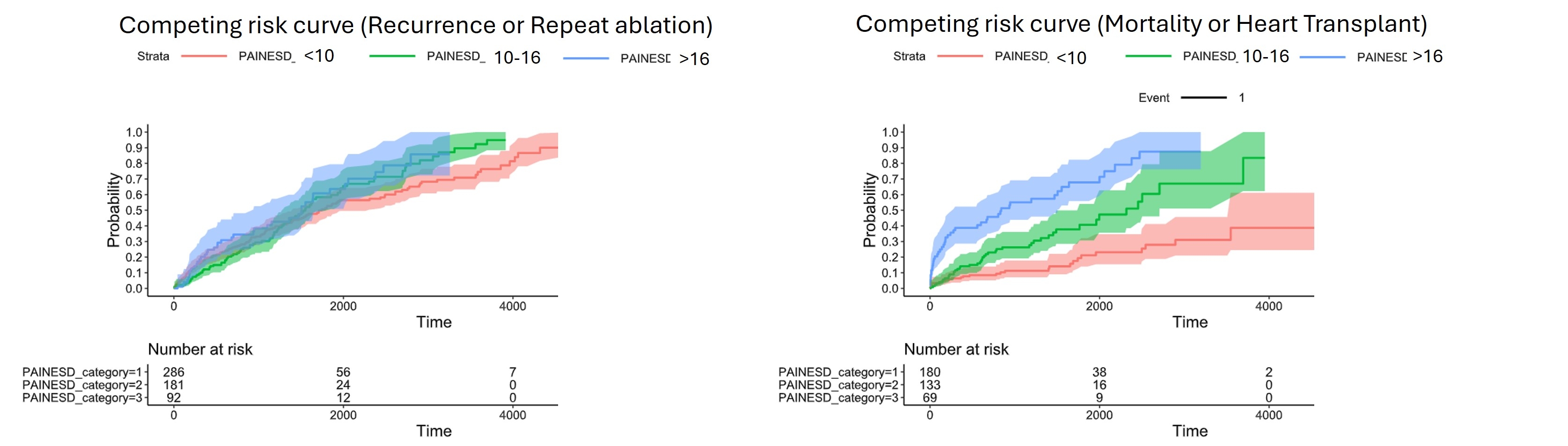
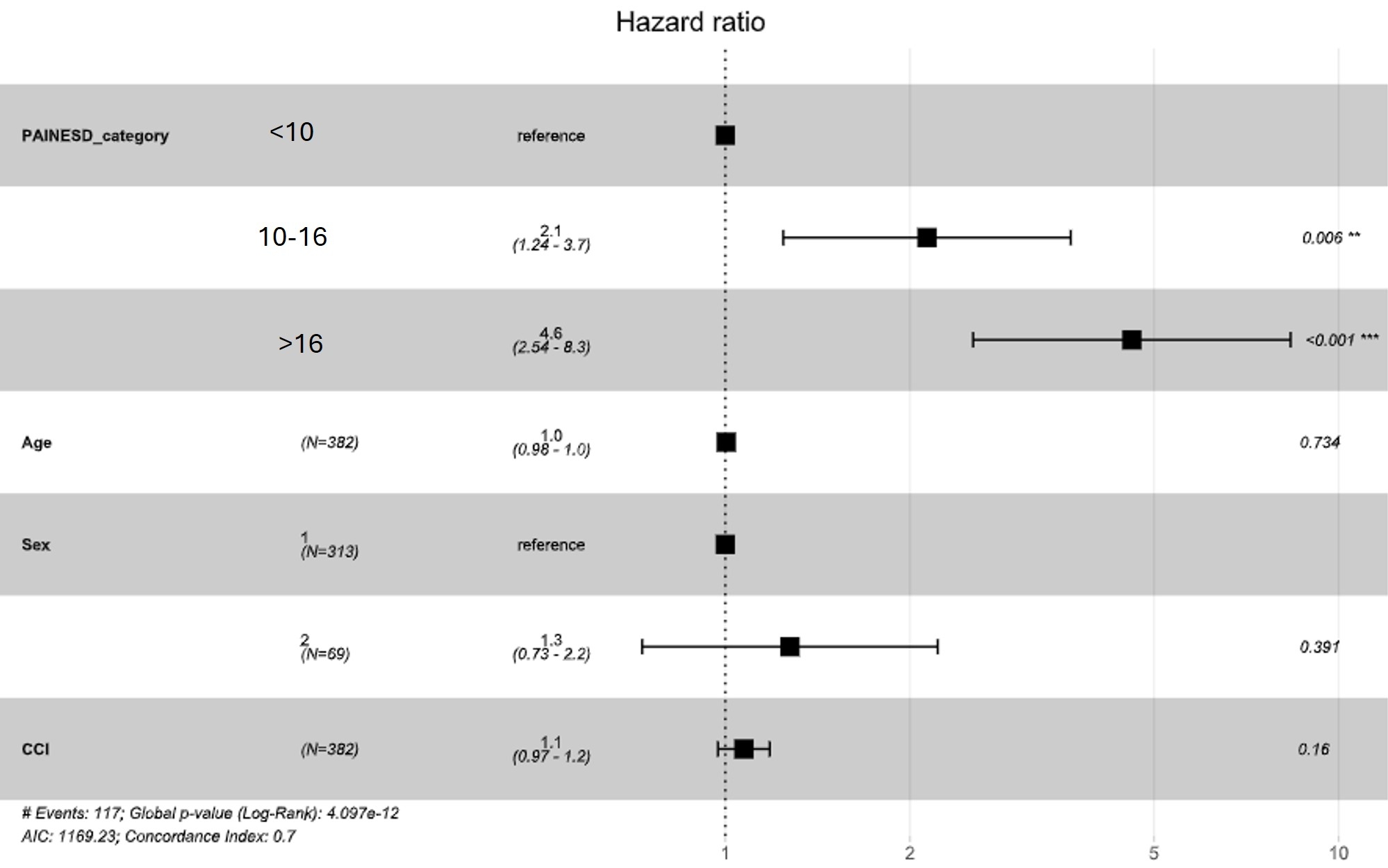
Abstract Body (Do not enter title and authors here): Background: PAINESD score was established as a predictor of periprocedural acute hemodynamic instability, long-term mortality and heart failure among patients undergoing catheter ablation for ventricular tachycardia (VT-CA). Objective: To assess the validity of PAINESD score and compare outcomes of high-risk patients undergoing catheter ablation for ventricular tachycardia (VT) with and without mechanical circulatory support (MCS) use during procedure. Methods: We conducted an observational dual-center study of consecutive patients with SHD undergoing VT-CA over a decade (2012-2022). The PAINESD score, based on 7 variables (COPD, age >60 years, general anesthesia, ischemic cardiomyopathy, NYHA class III or IV, ejection fraction <25%, VT storm, and diabetes mellitus), was calculated and categorized into low risk (<10), intermediate risk (10-16), and high risk (>16) as previously reported. Two survival analyses were performed to compare outcomes between different groups: one using all-cause mortality or heart transplant as the event, and another using recurrent or repeat ablation as the event. Multivariable Cox proportional hazards regression models were used to calculate hazard ratios for each PAINESD category and to determine the hazard ratio for the use of MCS among high-risk patients. Results: We found that between 2012 to 2022, 559 ablations were performed on 441 patients. There were 296 (53%), 182 (32.6%) and 81(14.5%) patients in low, medium, and high risk. Using low risk as reference, aHR for medium risk was 2.1 (1.24-3.7; p=0.006) and for high risk was 4.6(2.54-8.3; p <0.001). Among patients with high PAINESD score (n=81), 5 patients (6.2%) required MCS (Intra-arterial balloon pump (IABP)=1, ECMO only=1, ECMO+IABP=1, bypass=2). 4/5 (80%) patients on MCS stayed on them post procedure, except one patient on IABP. In this cohort, there was no difference between patients with and without MCS in primary outcome [aHR= 1.6 (0.48-5.4); p=0.43] and in secondary OUTCOME [1.29 (0.3-5.5; p=0.735)]. Conclusion: PAINESD was a significant predictor of mortality or heart failure, but it did not help in prediction of recurrence of VT, or repeat VT-CA.
Woelber, Tiffany
(
Mayo Clinic
, Rochester , Minnesota , United States )
Futela, Pragyat
(
MetroHealth Medical Center
, Cleveland , Ohio , United States )
Arunachalam Karikalan, Suganya
(
Mayo Clinic
, Rochester , Minnesota , United States )
Poddar, Aastha
(
Mayo Clinic
, Rochester , Minnesota , United States )
Heybati, Kiyan
(
Mayo Clinic
, Jacksonville , Florida , United States )
Pradeep, Aishwarya
(
Mayo Clinic
, Rochester , Minnesota , United States )
Prasitlumkum, Narut
(
Mayo Clinic
, Rochester , Minnesota , United States )
Amin, Hina
(
Mayo Clinic
, Rochester , Minnesota , United States )
Deshmukh, Abhishek
(
Mayo Clinic
, Rochester , Minnesota , United States )
Kowlgi, Gurukripa
(
Mayo Clinic
, Rochester , Minnesota , United States )
Author Disclosures:
Tiffany Woelber:DO NOT have relevant financial relationships
| Gurukripa Kowlgi:DO NOT have relevant financial relationships
| Pragyat Futela:DO NOT have relevant financial relationships
| Suganya Arunachalam Karikalan:No Answer
| Aastha Poddar:DO NOT have relevant financial relationships
| Kiyan Heybati:DO NOT have relevant financial relationships
| Aishwarya Pradeep:DO NOT have relevant financial relationships
| Narut Prasitlumkum:No Answer
| Hina Amin:No Answer
| Abhishek Deshmukh:DO NOT have relevant financial relationships