Outcome of Impella vs. Other Temporary Mechanical Circulatory Support Devices in Acute Myocardial Infarction Patients with Cardiogenic Shock: A Bayesian Network Meta-Analysis
Abstract Body (Do not enter title and authors here): Background: Cardiogenic shock (CS) affects up to 10% of hospitalized patients with acute myocardial infarction (AMI), leading to over 30% mortality despite treatment. In patients with AMI-CS refractory to vasopressors and inotropes, temporary mechanical circulatory support (MCS) devices have been used to provide hemodynamic support. Recently, Impella demonstrated significant mortality benefit in AMI-CS in the DanGer shock trial. However, it has not demonstrated such benefit over other devices, such as IABP and ECMO in other trials (ISAR-Shock, IMPRESS in Severe Shock, IMPELLA-STIC). Here we performed this network meta-analysis of all available studies including the DanGer shock trial comparing Impella with other MCS devices in AMI-CS patients.
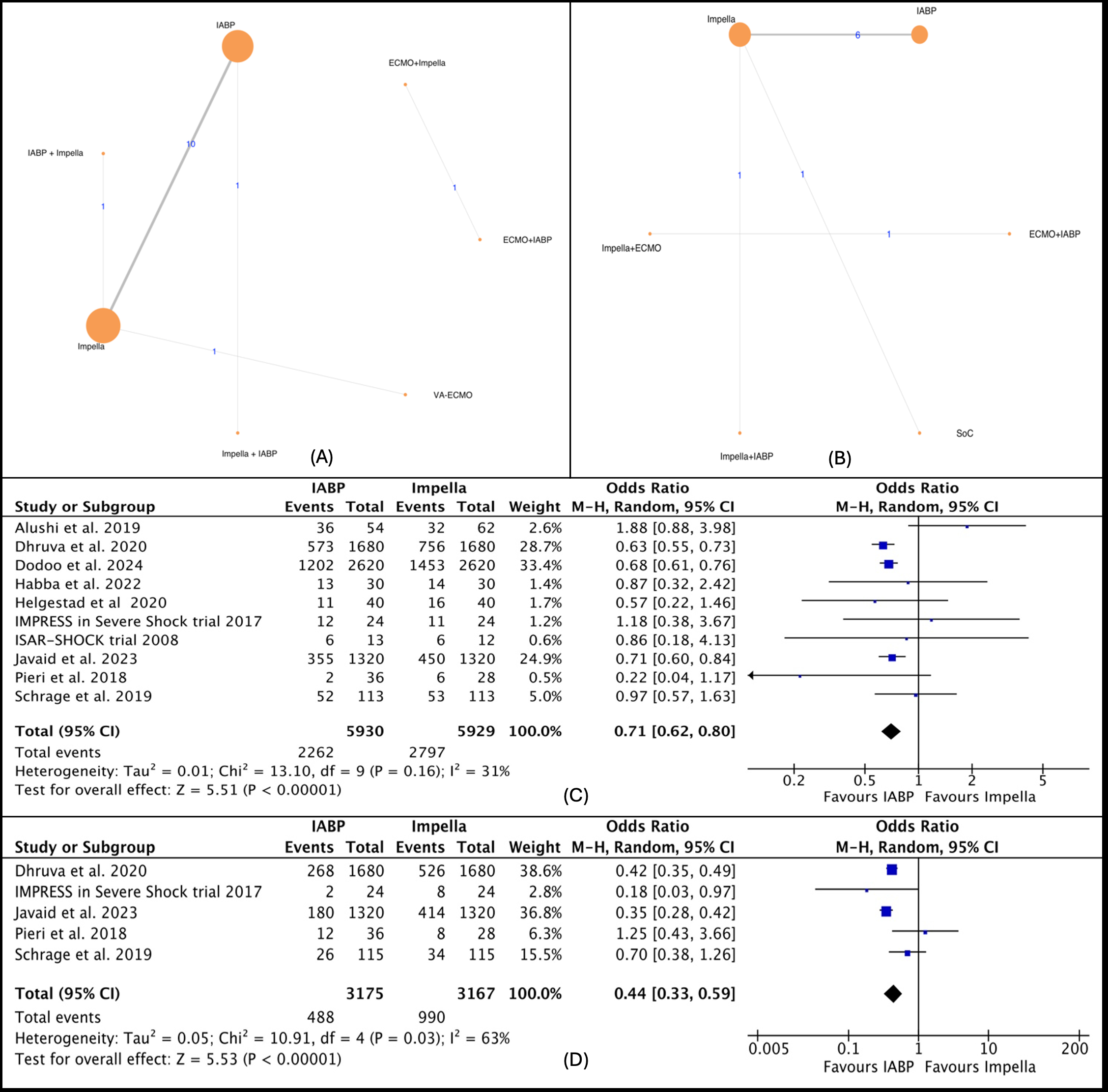
Method: We performed a Bayesian network meta-analysis to synthesize direct and indirect evidence from relevant studies published until April 2024 using PubMed, Embase, and Scopus databases comparing Impella with other strategies for treating AMI-CS patients. The primary outcome was a short-term mortality defined as in-hospital or 30-day mortality. This study is registered with PROSPERO, and data analysis was performed using the “BUGSnet” package in R.
Result: Out of 7,211 studies, 17 were deemed eligible. These included five RCTs and 12 observational studies, encompassing 16,654 patients with AMI-CS assigned to 3 different MSC interventions: Impella, IABP, and ECMO in 9 different combinations or alone. Based on SUCRA value, IABP was the most effective strategy in regard to short-term mortality (73.46), long-term mortality (75.59), major bleeding (66.4), renal replacement therapy (73.02); Impella along with IABP for stroke (95.24), ischemic stroke (99.68), device-related bleeding (90.22), MI (94.38); ECMO for hemolysis (91.66); standard of care for peripheral ischemic complications (88.66), sepsis (78.71). In sub-analysis using the RCTs only, Impella was ranked best for short-term mortality (74.53).
Conclusion: Based on the findings of this network meta-analysis, IABP could potentially provide both short-term and long-term mortality benefits, as well as reduce the risk of bleeding. Meanwhile, combining it with Impella could potentially reduce the risk of cerebral ischemia.
Oli, Prakash
(
Mount Sinai Hospital
, Chicago , Illinois , United States )
Shrestha, Dhan
(
Bassett Medical Centre
, Cooperstown , New York , United States )
Lamichhane, Sandesh
(
Chitwan Medical College
, Chitwan , Nepal )
Shrestha, Swikriti
(
Chitwan Medical College
, Chitwan , Nepal )
Kansakar, Sajog
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Shtembari, Jurgen
(
Carle Foundation
, Chicago , Illinois , United States )
Dawadi, Sagun
(
Nepalese Army Institute of Health Sciences
, Kathmandu , Nepal )
Katz, Daniel
(
Basset Healthcare
, Cooperstown , New York , United States )
Author Disclosures:
Prakash Oli:DO NOT have relevant financial relationships
| Dhan Shrestha:DO NOT have relevant financial relationships
| Sandesh Lamichhane:DO NOT have relevant financial relationships
| Subash Subedi:DO NOT have relevant financial relationships
| Swikriti Shrestha:DO NOT have relevant financial relationships
| Sajog Kansakar:DO NOT have relevant financial relationships
| Jurgen Shtembari:DO NOT have relevant financial relationships
| Sagun Dawadi:DO NOT have relevant financial relationships
| Daniel Katz:DO NOT have relevant financial relationships