Bonnie and Clyde: Pulmonary artery aneurysm with concomitant ascending aortic aneurysm
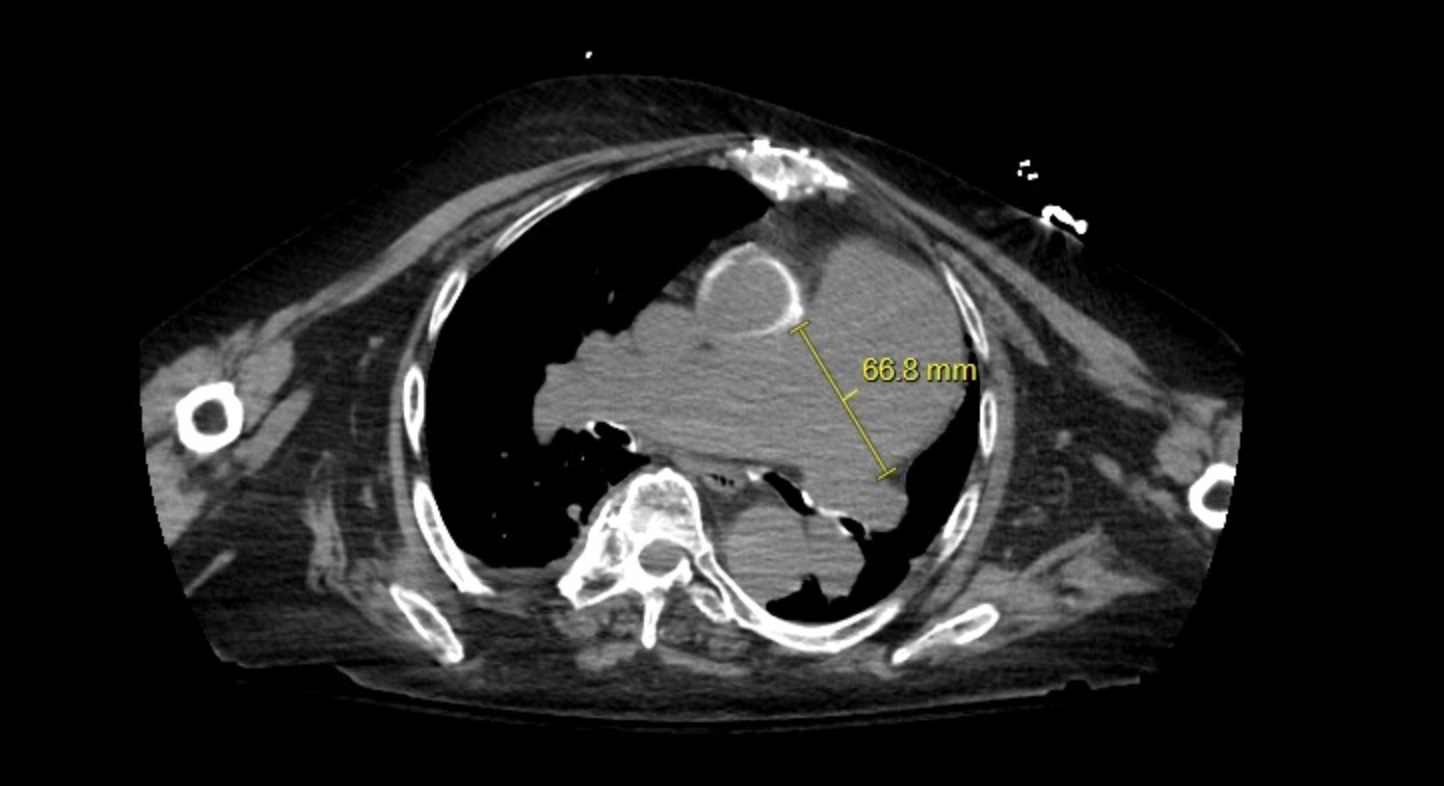
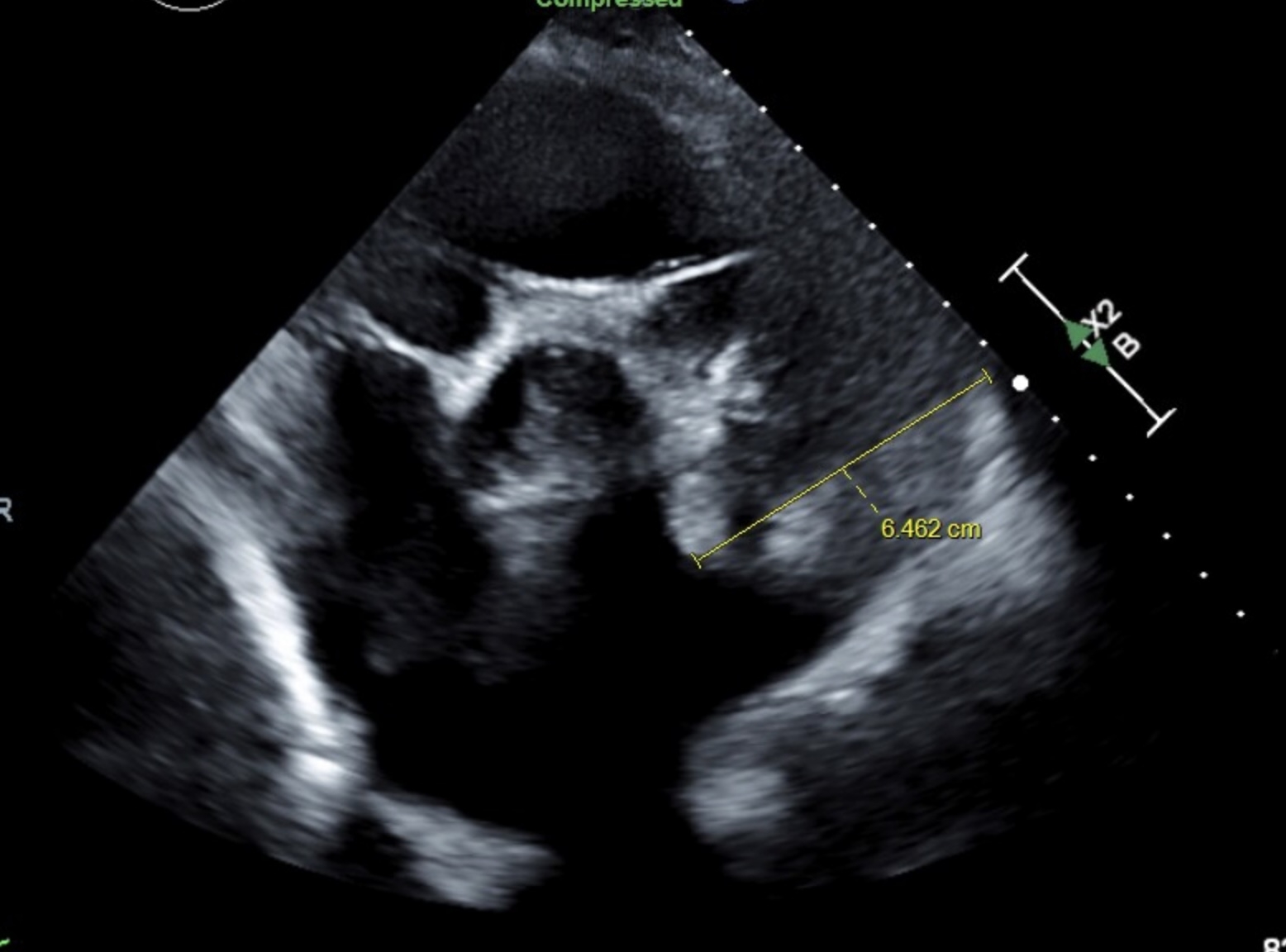
Abstract Body (Do not enter title and authors here): Background: Pulmonary artery aneurysms (PAAs) are rare with an incidence of 1 in 14,000. While rare, they are very critical conditions with a mortality rate of 50-100%. PAAs may be congenital or acquired via infections, vasculitis, pulmonary arterial hypertension, chronic pulmonary embolism, inflammatory lung disease, neoplasm, or iatrogenic. The risk of PAA is due to respiratory compromise, compression of other structures, and dissection. We describe the rare presentation of a PAA with a concomitant ascending aortic aneurysm. Case Description: 75-year-old woman with a PMH of hypertension, Group I pulmonary artery hypertension, HFpEF, non-obstructive CAD, aortic insufficiency s/p mechanical aortic valve replacement on warfarin since 02/2014, hyperlipidemia who was admitted due to altered mental status. Physical exam was remarkable for 4/6 diastolic murmur, 3/6 aortic murmur, prominent P2, and parasternal lift and no JVD or lower extremity edema. CXR incidentally showed enlarged pulmonary artery and CT chest showed PAA at 6.6 cm. Echocardiogram confirmed moderate to severe pulmonary hypertension and a markedly dilated PAA with pulmonary valvular insufficiency. In addition, she had an ascending aortic aneurysm with moderate aortic insufficiency. The two coinciding aneurysms could be distinct in etiology due to sequela of high pressure vessel wall degradation from pulmonary artery hypertension and systemic hypertension or related due to vasculitis or cystic medial necrosis/connective tissue disease. Due to multiple concomitant aneurysms, the patient is pending further workup. Discussion: Aneurysms are focal dilations with PAA larger than 29 mm and ascending aortic aneurysm larger than 44 mm. Common etiologies include vasculitis, connective tissue disease, and high vessel pressure. Due to the risk of fatal pulmonary hemorrhage, PAAs are critical. Diagnosis of PAA is via CTA and of aortic aneurysm is via TTE with annual monitoring. Surgical intervention is greater than 45-55 mm depending on risk factors for ascending aortic aneurysm and greater than 55 mm for PAA. Surgical interventions for PAAs include stent graft, aneurysmorrhaphy, lobectomy, aneurysmectomy, and pneumonectomy. Surgical resection comes with high risk in patients with severe pulmonary hypertension. Treating the underlying pulmonary artery hypertension is crucial to long term management along with determination and treatment of underlying cause.
Sandhu, Hasnoor
(
Franciscan Health Olympia Fields
, Aurora , Illinois , United States )
Marrium, Areeba
(
Franciscan Health Olympia Fields
, Aurora , Illinois , United States )
Shadrix, Alyson
(
Franciscan Health Olympia Fields
, Aurora , Illinois , United States )
Kumar, Amit
(
Franciscan Health Olympia Fields
, Aurora , Illinois , United States )
Hamoui, Omar
(
Franciscan Health Olympia Fields
, Aurora , Illinois , United States )
Author Disclosures:
Hasnoor Sandhu:DO NOT have relevant financial relationships
| Areeba Marrium:DO NOT have relevant financial relationships
| Alyson Shadrix:DO NOT have relevant financial relationships
| Amit Kumar:No Answer
| Omar Hamoui:No Answer